Dementia Risk in Type 2 Diabetes Patients: Acarbose Use and Its Joint Effects with Metformin and Pioglitazone
Tseng Chin-Hsiao1, 2, 3, *
1Department of Internal Medicine, National Taiwan University College of Medicine, Taipei, Taiwan2Division of Endocrinology and Metabolism, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan3Division of Environmental Health and Occupational Medicine of the National Health Research Institutes, Zhunan, Taiwan
通讯作者: Correspondence should be addressed to: Dr. Chin-Hsiao Tseng, Department of Internal Medicine, National Taiwan University HospitalTaipei (100), Taiwan. E-mail: ccktsh@ms6.hinet.net.
收稿日期:2019-03-4
修回日期: 2019-06-18
接受日期: 2019-06-21
网络出版日期: 2020-05-09
版权声明:
2020 This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium provided that the original work is properly attributed.
展开
Abstract
This population-based retrospective cohort study investigated dementia risk associated with acarbose in patients with type 2 diabetes mellitus by using Taiwan’s National Health Insurance database. A cohort of 15,524 matched pairs of ever and never users of acarbose based on propensity score matching was enrolled from new-onset type 2 diabetes patients from 1999 to 2006. Patients who were alive on January 1, 2007, were followed up for dementia until December 31, 2011. Adjusted hazard ratios were estimated using Cox proportional hazards models. The results revealed that the incident case numbers (incidence rates) of dementia were 264 (407.19 per 100,000 person-years) for never users and 231 (337.94 per 100,000 person-years) for ever users. The hazard ratio for ever users versus never users was 0.841 (95% confidence interval, 0.704-1.005) and 0.918 (0.845-0.998) for every 1-year increment of cumulative duration of acarbose therapy. Subgroup analyses showed that the reduced risk associated with acarbose was only observed in women (adjusted hazard ratio, 0.783; 95% confidence interval, 0.618-0.992) and in non-users of metformin (adjusted hazard ratio, 0.635; 95% confidence interval, 0.481-0.837). A model comparing different combinations of acarbose, metformin, and pioglitazone suggested that users of all three drugs had the lowest risk of dementia (hazard ratio, 0.406; 95% confidence interval, 0.178-0.925). In conclusion, reduced risk of dementia associated with acarbose is observed in the female sex and in non-users of metformin. Moreover, users of all three drugs (acarbose, metformin, and pioglitazone) have the lowest risk of dementia.
TsengChin-Hsiao. Dementia Risk in Type 2 Diabetes Patients: Acarbose Use and Its Joint Effects with Metformin and Pioglitazone[J]. Aging and Disease, 2020, 11(3): 658-667 https://doi.org/10.14336/AD.2019.0621
Dementia can either have a vascular etiology or occur because of a neurodegenerative disease such as Alzheimer’s disease (AD). Diabetes patients have a significantly 5-fold increased risk of dementia [1]. The close association between type 2 diabetes mellitus and AD and their potential common pathophysiological changes of impaired insulin expression and insulin resistance led to the coining of the term “type 3 diabetes” for AD [2]. The increased risk of dementia in diabetes patients may be due to the increased incidence of atherosclerosis, blood-brain barrier disturbances, and neurodegeneration associated with diabetes mellitus. The pathophysiological changes may include insulin resistance, increased deposition of advanced glycation end products, dysregulation of lipid metabolism, and augmented inflammation and oxidative stress [1,3]. Studies also suggest that postprandial glucose and glucose variability may increase the risk of cognitive dysfunction and dementia [4,5].
Major brain pathological changes of AD include deposition of amyloid beta (Aβ) and hyper-phosphorylation of tau protein [2]. Aβ is formed by the cleaving of the amyloid precursor protein by secretases [6], and insulin resistance in the brain may aggravate the accumulation of Aβ [7]. Additionally, AD is characterized by neurodegeneration with damage in cholinergic neurons, resulting in reduced release of acetylcholine neurotransmitters [8]. Acetylcholinesterase and butyryl-cholinesterase are serine hydrolases that are responsible for the catalytic hydrolysis of acetylcholine and they play an important role in the aggregation of Aβ [9]. Therefore, cholinesterase inhibitors are the main drugs currently approved for AD treatment [8,10].
Theoretically, antidiabetic drugs that improve insulin resistance in the brain can potentially prevent AD or dementia [2]. As shown in our previous observational studies, two antidiabetic drugs, specifically metformin [11] and pioglitazone [12], that improve insulin resistance, show a reduced risk of dementia in a dose-response pattern in patients with type 2 diabetes mellitus.
Acarbose, an alpha-glucosidase inhibitor that inhibits the digestion of carbohydrate in the intestine, is commonly used to treat diabetes in Asian populations, probably because of its glucose lowering effect for patients who consume Asian diets that have a high content of carbohydrate [13,14]. Acarbose has the following benefits that may contribute to a reduction of dementia risk: lowering postprandial glucose with a lower risk of hypoglycemia, improving insulin resistance, improving lipid profile, enhancing the release of glucagon-like peptide-1, inhibiting platelet activation, exerting anti-inflammatory effect, and reducing oxidative stress [13,15]. Indeed, novel drugs that may exert inhibitory effects on alpha glucosidase and cholinesterase are being developed for the treatment of both type 2 diabetes mellitus and AD [16].
A recent animal study suggested that acarbose has a protective effect on the decline of cognitive function, including spatial learning and memory, in SAMP8 mice [17]. However, a recent small scale randomized clinical trial conducted in patients with non-dementia vascular cognitive impairment and abnormal glucose metabolism showed an improvement in cognitive function only in patients assigned to metformin and donepezil (n = 50) for one year but not in those assigned to acarbose and donepezil (n = 50) [18]. Whether prolonged use of acarbose in diabetes treatment might exert a potential benefit for dementia has not been investigated. The present study investigated dementia risk in patients with type 2 diabetes mellitus who had been treated with acarbose and those who had never been treated with acarbose in the Chinese population in Taiwan by using the reimbursement database of the National Health Insurance (NHI).
MATERIALS AND METHODS
This retrospective cohort study used the longitudinal reimbursement database of Taiwan’s NHI. The NHI is a unique healthcare system that covers more than 99.6% of Taiwan’s population; it has been implemented since March 1995. A majority of medical institutions throughout the nation (93%) have been contracted to the Bureau of NHI. The database keeps records of all disease diagnoses, medication prescriptions, and performed procedures. This can be used for academic research after ethics review.
The approval number for the present study was 99274 by the National Health Research Institutes and the database was described in detail in previous papers [19,20]. Throughout the study period, diabetes was coded 250.XX according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) and dementia was coded as abridged codes of A210 or A222, or as ICD-9-CM codes of 290.0, 290.1, 290.2, 290.4, 294.1, 331.0-331.2, or 331.7-331.9.
The procedures used to create a cohort of 1:1 matched pair of ever users and never users of acarbose are shown in Figure 1. At first, 446,105 patients who had new-onset diabetes mellitus from 1999 to 2006 and who had been prescribed antidiabetic drugs two or more times were identified from the outpatient clinics. Patients diagnosed with diabetes mellitus between 1996 and 1998 were excluded to ensure that only patients with new-onset diabetes were included in the study. The following patients were then excluded: 1) patients who had been diagnosed with dementia and/or died before January 1, 2007 (n = 25,565); 2) patients who were initiated with acarbose after January 1, 2007 (n = 81,689); 3) patients with type 1 diabetes mellitus (n = 2263); 4) patients with missing data (n = 493); 5) patients who had used acarbose for <180 days (n = 15,336); 6) patients with a diagnosis of any cancer before entry (n = 35,251, cancer patients were excluded because they might have shortened lifespans which might have distorted follow-up time and dementia could be misdiagnosed from the clinical presentations of malignancy); 7) patients aged <25 years (n = 1192); 8) patients aged >75 years (n = 32,570); 9) patients with Parkinson’s disease before entry (n = 2718); 10) patients with head injury before entry (n = 3158); 11) patients with a diagnosis of hypoglycemia before entry (n = 2337); 12) patients with a history of stroke before entry (n = 43,178); and 13) patients with a follow-up duration < 180 days (n = 4675). Patients with Parkinson’s disease, head injury, hypoglycemia, and stroke were excluded because these diagnoses are important risk factors for dementia. As a result, 15,566 ever users and 180,114 never users of acarbose were identified (unmatched original cohort). A cohort of 1:1 matched pairs of 15,524 ever users and 15,524 never users (the matched cohort) was created by propensity score matching based on the Greedy 8→1 digit match algorithm [21]. Logistic regression was used to create the propensity score from all characteristics listed in Table 1 being treated as independent variables.
Figure 1. Flowchart for the procedures in selecting a propensity score-matched cohort of acarbose ever users and never users.
The cumulative duration of acarbose therapy in years was calculated from the database. Potential confounders included the following categories: demographic data, major comorbidities associated with diabetes mellitus, diabetes-related complications, potential risk factors for cancer, potential factors that may affect the prescription of acarbose, antidiabetic drugs, and medications commonly used in diabetes patients. Demographic data included age, sex, diabetes duration, occupation, and living region (classified as Taipei, Northern, Central, Southern, and Kao-Ping/Eastern). Occupation was classified as class I (civil servants, teachers, government employees or private businesses, professionals, and technicians), class II (people without a specific employer, self-employed people, or seamen), class III (farmers or fishermen) and class IV (low-income families supported by social welfare, or veterans). The ICD-9-CM codes for potential confounders categorized as major comorbidities associated with diabetes mellitus (hypertension, dyslipi-demia, and obesity), diabetes-related complications (nephropathy, eye disease, ischemic heart disease, and peripheral arterial disease), potential risk factors for cancer (chronic obstructive pulmonary disease, tobacco abuse, and alcohol-related diagnoses), and potential factors that may affect the prescription of acarbose (gallstone, diseases of the digestive system, Helicobacter Pylori infection, and/or Helicobacter Pylori eradication therapies, hepatitis B virus infection, hepatitis C virus infection, liver cirrhosis, and other chronic non-alcoholic liver diseases) can be found in previously published papers [11,12,22]. Antidiabetic drugs included insulin, sulfonylurea, metformin, meglitinide, rosiglitazone, and pioglitazone. Commonly used medications in diabetes patients included angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, calcium channel blockers, statins, fibrates, and aspirin.
Student’s t test was used to compare the differences of age and diabetes duration between never and ever users and the Chi-square test was used for other variables. According to Austin and Stuart, a standardized difference was calculated for each covariate and a cutoff value of >10% was used as an indicator of potential confounding from the variable [23].
Because previous animal studies showed that acarbose may exert a better anti-aging effect in male mice than in female mice [24] and the use of either metformin [11] or pioglitazone [12] may reduce the risk of dementia, the incidence density of dementia was calculated for ever users and never users of acarbose in all patients and in subgroups of men, women, patients with metformin use, patients without metformin use, patients with pioglitazone use and patients without pioglitazone use, respectively, and for different subgroups of combinations of the use of acarbose, metformin and pioglitazone. The numerator was the number of newly diagnosed cases of dementia patients identified during follow-up and the denominator was the follow-up duration in person-years. Follow-up started on January 1, 2007, and ended on December 31, 2011, at the time of a new diagnosis of dementia, or on the date of death or the last reimbursement record, whichever occurred first.
Cox proportional hazards model was used to estimate the adjusted hazard ratios and their 95% confidence intervals for ever users versus never users of acarbose, and for the cumulative duration (every 1-year increment) of acarbose therapy being treated as a continuous variable in all patients, and in men and women, respectively. To evaluate the effects of acarbose in the presence or absence of metformin or pioglitazone, hazard ratios for acarbose ever users versus never users were estimated in subgroups of patients with metformin use, without metformin use, with pioglitazone use and without pioglitazone use, respectively. Finally, the joint effects of the use of acarbose, metformin, and pioglitazone were evaluated in a model that estimated the hazard ratios in different subgroups of all possible combinations of the use of the three drugs by using a referent group including patients without the use of any of the three drugs. All baseline characteristics were considered as potential confounders and were adjusted for in the aforementioned Cox proportional hazards models.
Kaplan-Meier curves for dementia-free probability were plotted for acarbose never users versus ever users in all patients, in men, in women and in different subgroups of all possible combinations of the use of acarbose, metformin, and pioglitazone. Logrank test was used to test the significance among different subgroups of acarbose exposure.
Analyses were conducted using SAS Version 9.4 (SAS Institute, Cary, NC). P-value < 0.05 was considered statistically significant.
Table 1
Table 1 Characteristics in never and ever users of acarbose.
Variable
Never users
Ever users
(n=15524)
(n=15524)
P-value
Standardized difference
n
%
n
%
Demographic data
Age (years)
59.76
10.10
59.75
9.95
0.9225
-0.13
Sex (men)
8358
53.84
8443
54.39
0.3330
1.15
Diabetes duration (years)
5.42
2.41
5.45
2.27
0.2444
1.26
Occupation
I
6749
43.47
6782
43.69
0.6102
II
3687
23.75
3609
23.25
-1.24
III
2515
16.20
2580
16.62
1.14
IV
2573
16.57
2553
16.45
-0.34
Living region
Taipei
5923
38.15
5884
37.90
0.6517
Northern
1859
11.98
1785
11.50
-1.55
Central
1859
11.98
2736
17.62
0.80
Southern
1962
12.64
1990
12.82
0.61
Kao-Ping and Eastern
3089
19.90
3129
20.16
0.70
Major comorbidities
Hypertension
10796
69.54
10777
69.42
0.8149
-0.34
Dyslipidemia
11515
74.18
11498
74.07
0.8256
-0.35
Obesity
1036
6.67
959
6.18
0.0747
-2.08
Diabetes-related complications
Nephropathy
2717
17.50
2729
17.58
0.8579
0.23
Eye disease
3864
24.89
3861
24.87
0.9686
0.01
Ischemic heart disease
5253
33.84
5234
33.72
0.8197
-0.34
Peripheral arterial disease
2642
17.02
2614
16.84
0.6718
-0.51
Potential risk factors of cancer
Chronic obstructive pulmonary disease
5657
36.44
5597
36.05
0.4787
-0.84
Tobacco abuse
385
2.48
385
2.48
0.3738
-1.07
Alcohol-related diagnoses
747
4.81
734
4.73
0.7292
-0.45
Potential factors that may affect the prescription of acarbose
Table 1 shows the characteristics of never users and ever users of acarbose. None of the calculated values of standardized difference between the two groups was found to be > 10%, suggesting that the two groups were well matched in these covariates. However, the proportion of liver cirrhosis in ever users was slightly higher than that in never users (3.17% versus 2.71%, P-value = 0.0171).
The incidence rates of dementia and the adjusted hazard ratios by acarbose exposure in all patients and in different sexes are shown in Table 2. In all patients, the adjusted hazard ratio comparing acarbose ever users versus never users suggested a non-significant risk reduction associated with acarbose use (adjusted hazard ratio, 0.841; 95% confidence interval, 0.704-1.005). When treated as a continuous variable, the cumulative duration of acarbose therapy was significantly associated with a reduced risk. In the analyses conducted in men and women separately, acarbose showed a neutral effect in men but a protective effect in women.
Table 3 shows the results of models analyzing the effects of acarbose on dementia risk with regard to exposure to metformin and/or pioglitazone. The findings suggested that the reduced risk of dementia associated with acarbose use was mainly observed in non-users of metformin (model II) and was not significantly observed in patients who were using metformin (model I). The use (model III) or non-use of pioglitazone (model IV) did not significantly affect the risk of dementia associated with acarbose. In the model evaluating the joint effects of all possible combinations of the use of acarbose, metformin, and pioglitazone (model V), patients who were using all the three drugs (group 7) showed a significantly low risk of dementia. Patients who were using one or two of the three drugs showed either a non-significant association (groups 2, 3. and 6) or a significant risk reduction (groups 1, 4, and 5).
Table 2
Table 2 Incidence rates of dementia and hazard ratios by acarbose exposure in all patients and in different sexes.
Models
n
N
Person-years
Incidence rate (per 100,000 person-years)
Adjusted hazard ratio
95% Confidence interval
P-value
All patients
Acarbose never users
264
15524
64834.36
407.19
1.000
Acarbose ever users
231
15524
68355.38
337.94
0.841
(0.704-1.005)
0.0561
Cumulative duration of acarbose therapy treated as a continuous variable
For every 1-year increment of acarbose use
0.918
(0.845-0.998)
0.0444
Men
Acarbose never users
101
8358
34603.53
291.88
1.000
Acarbose ever users
107
8443
37111.21
288.32
0.934
(0.710-1.228)
0.6252
Cumulative duration of acarbose therapy treated as a continuous variable
For every 1-year increment of acarbose use
0.983
(0.871-1.110)
0.7840
Women
Acarbose never users
163
7166
30230.84
539.18
1.000
Acarbose ever users
124
7081
31244.17
396.87
0.783
(0.618-0.992)
0.0425
Cumulative duration of acarbose therapy treated as a continuous variable
Kaplan-Meier curves comparing dementia-free probability in different subgroups of acarbose exposure are shown in Figure 2. Figure 2A, 2B and 2C compare ever and never users of acarbose in all patients (logrank P-value = 0.0268), in men (logrank P-value = 0.8516), and in women (logrank P-value = 0.0076), respectively. Figure 2D compares the dementia-free probability among the subgroups of different combinations of the use of acarbose, metformin, and pioglitazone. The logrank test (P-value < 0.0001) suggested a significant difference among the subgroups and patients who were using all three drugs had the lowest risk of developing dementia.
DISCUSSION
The findings suggested that acarbose use in patients with type 2 diabetes mellitus might exert some protective effect against dementia (Table 2), and that such a benefit was mainly observed in female patients (Table 2 and Figure 2C) and in non-users of metformin (model II of Table 3). In the analyses of the joint effects of acarbose, metformin and pioglitazone, the lowest risk of dementia was observed in those who were using all three drugs (group 7 in model V of Table 3 and Figure 2D).
As shown in our previous studies, metformin [11] and pioglitazone [12] improve insulin resistance and are associated with a lower risk of dementia. This study provided information to support the potential role of insulin resistance in dementia in patients with type 2 diabetes mellitus because acarbose may also reduce insulin resistance, though to a lesser extent. However, unlike metformin and pioglitazone that may pass through the blood-brain barrier [11,12], acarbose or its metabolites do not cross the blood-brain barrier [24]. Therefore, acarbose may not act directly on the central nervous system. Acarbose is especially useful for reducing postprandial glucose and it is less likely to cause hypoglycemia [13,15]. Therefore, the reduced oxidative stress because of reduced glucose variability in patients treated with acarbose may contribute to a reduced risk of dementia. The improvement of lipid profile, inhibition of platelet activation, and the reduction of inflammation associated with acarbose use [13,15] may also partly explain the reduced risk of dementia associated with acarbose.
Figure 2. Kaplan-Meier curves comparing dementia-free probability in different subgroups of acarbose exposure. Kaplan-Meier curves comparing dementia-free probability between ever users and never users of acarbose in both sexes together (A) and in separate sexes (B: men, C: women). (D) compares the respective curves in subgroups of patients with different combinations of use (+) and non-use (-) of metformin (M), pioglitazone (P) and acarbose (A). The 95% confidence intervals are shown in shaded areas. HR: hazard ratio; CI: confidence interval.
The subgroup analyses suggested that the beneficial effect of acarbose on dementia was mainly observed in female patients (Table 2) and in non-users of metformin (model II of Table 3). Metformin is protective against dementia per se [11] and it is always used as a first-line treatment for type 2 diabetes mellitus. Therefore, patients who used both metformin and acarbose in the study might have been benefited from the protection against dementia by metformin and the benefit of acarbose might not be additive to the effect of metformin. It is worthy to note that the beneficial effect of metformin on dementia could also be demonstrated in the present study by comparing the incidence rates of dementia in patients who were using metformin versus those who were not using metformin in never users of acarbose (332.42 versus 523.07 per 100,000 person-years) and in ever users of acarbose (309.78 versus 380.13 per 100,000 person-years), respectively (Models I and II of Table 3). Similarly, female patients seemed to suffer from a higher incidence of dementia than male patients in acarbose never users and ever users, respectively (Table 2).
The differential effects of acarbose on dementia risk in male and female patients are interesting. Previous animal studies also suggested differential effects of acarbose on lifespan prolongation in male and female mice [24]. While acarbose increased the median lifespan by 22% in male mice (P-value < 0.0001), it increased the lifespan in female mice by only 5% (P-value = 0.01) [24]. Although acarbose was beneficial in prolonging the lifespan in male mice [24], its benefit on dementia seemed to be more predominant in the female patients in the present study (Table 2). The reason for such a discrepancy between different sexes in terms of lifespan in mice and in terms of dementia in humans remains unknown.
Table 3
Table 3 The effects of acarbose on dementia risk with regards to exposure to metformin and/or pioglitazone.
Models
n
N
Person-years
Incidence rate (per 100,000 person-years)
Adjusted hazard ratio
95% Confidence interval
P-value
1.Patients with metformin
Acarbose never users
131
9374
39407.59
332.42
1.000
Acarbose ever users
127
9370
40996.20
309.78
1.023
(0.798-1.312)
0.8559
2.Patients without metformin
Acarbose never users
133
6150
25426.78
523.07
1.000
Acarbose ever users
104
6154
27359.18
380.13
0.635
(0.481-0.837)
0.0013
3.Patients with pioglitazone
Acarbose never users
27
1397
6101.85
442.49
1.000
Acarbose ever users
13
1415
6098.01
213.18
0.598
(0.303-1.180)
0.1382
4.Patients without pioglitazone
Acarbose never users
237
14127
58732.51
403.52
1.000
Acarbose ever users
218
14109
62257.37
350.16
0.877
(0.728-1.055)
0.1644
5.Joint effects of metformin, pioglitazone and acarbose
Group 0: Metformin (-) / Pioglitazone (-) / Acarbose (-)
126
5647
23323.77
540.22
1.000
Group 1: Metformin (-) / Pioglitazone (-) / Acarbose (+)
97
5600
24953.18
388.73
0.643
(0.489-0.845)
0.0015
Group 2: Metformin (-) / Pioglitazone (+) / Acarbose (-)
7
503
2103.01
332.86
0.635
(0.295-1.369)
0.2466
Group 3: Metformin (-) / Pioglitazone (+) / Acarbose (+)
7
554
2405.99
290.94
0.603
(0.281-1.295)
0.1945
Group 4: Metformin (+) / Pioglitazone (-) / Acarbose (-)
111
8480
35408.74
313.48
0.596
(0.457-0.779)
0.0002
Group 5: Metformin (+) / Pioglitazone (-) / Acarbose (+)
121
8509
37304.19
324.36
0.691
(0.535-0.893)
0.0048
Group 6: Metformin (+) / Pioglitazone (+) / Acarbose (-)
20
894
3998.85
500.14
1.104
(0.683-1.784)
0.6870
Group 7: Metformin (+) / Pioglitazone (+) / Acarbose (+)
In recent decades, there has been a dramatic increase in diabetes worldwide, and millions of patients are using antidiabetic drugs. This study may have some clinical and research significance because acarbose remains an important oral antidiabetic drug, especially in Asian populations. Although no definite beneficial effects on cardiovascular disease were observed with acarbose treatment in a clinical trial conducted in the Chinese population in China [25], the potential benefit of acarbose on dementia in specific subgroups of patients, i.e., in female patients (Table 2), in non-users of metformin (model II of Table 3) and in combination with metformin and pioglitazone (group 7 in model V of Table 3), provides rationale for repositioning acarbose in the treatment of Chinese patients with type 2 diabetes mellitus. At least, based on current evidence, acarbose may be considered in patients who consume large amounts of carbohydrate and it can be used as a substitute for metformin in patients who are at risk of dementia but contraindicated for metformin use or who cannot tolerate the side effects of metformin, especially in female patients. A combination of acarbose, metformin, and pioglitazone may be a good choice in some patients who require greater control of blood glucose. Such a combination theoretically provides a better glycemic control without the risk of hypoglycemia and with a much more reduced insulin resistance. The findings of the present study also provide rationale for the development of novel drugs that can pass through the blood-brain barrier and exert dual inhibitory effects on alpha glucosidase and cholinesterase for targeting the treatment of both type 2 diabetes mellitus and AD [16].
The present study has considered some potential biases commonly encountered in pharmaco-epidemiological studies that use pre-existing administrative databases. These biases include selection bias, prevalent user bias, immortal time bias, and confounding by indication. By using the nationwide database that covers more than 99.6% of the population, selection bias is not a problem. Because the patients should have had new-onset type 2 diabetes mellitus during the enrollment period and the use of acarbose was counted from the longitudinal database since its very first prescription, we included incident users of acarbose and avoided the potential risk of prevalent user bias.
Immortal time refers to the follow-up period when the outcome cannot occur. Therefore, immortal time bias can be introduced when the treatment status or follow-up time is inappropriately assigned [26]. In the present study, ambiguous diagnosis of diabetes was unlikely because only patients who had been prescribed antidiabetic drugs two or more times had been enrolled (Figure 1). Misclassification of treatment status was also unlikely in Taiwan because the NHI is a universal healthcare system and the information of all prescriptions was completely stored in computer files during the whole study period. Therefore, misdiagnosis of diabetes and misclassification of treatment status were well avoided.
The follow-up time of the patients was also carefully considered to avoid the inclusion of immortal time. First, immortal time bias was avoided by excluding patients who had a short follow-up period of < 180 days (Figure 1). The immortal time between diabetes diagnosis and the start of the use of antidiabetic drugs had been avoided because patients were enrolled only when they started with the treatment of antidiabetic drugs and immortal time was actually not calculated in the person-years. The immortal time introduced during the waiting period between the prescription and the dispensing of medications after hospital discharge as described by Lévesque et al. [26] would not occur in Taiwan because all discharge medications can be obtained directly from the hospital when the patients are discharged.
Confounding by indication could be reduced by using a cohort of propensity score-matched pairs of ever and never users of acarbose (Figure 1). Because none of the covariates had a standardized difference > 10% in the matched cohort (Table 1), residual confounding by indication was not likely. It was noted that the distribution of liver cirrhosis differed significantly between ever users and never users of acarbose (Table 1). However, this would probably not exert a confounding effect because the difference was small and such an effect has been adjusted for in the estimation of the hazard ratios (Tables 2 and 3).
Some other merits deserve mentioning. Because the NHI database covers > 99.6% of Taiwan’s population, the findings can be readily generalized to the whole population. The potential bias resulting from self-reporting could be further reduced by using medical records. Detection bias resulting from different socioeconomic statuses is less likely in our healthcare system because the drug cost sharing is low and can always be waived off for low-income patients, veterans, and prescription refills for chronic diseases.
The study limitations may include a lack of records of blood levels of glucose and insulin, a lack of glucose excursion index, a lack of indicators of insulin resistance, and β-cell function for more in-depth analyses. Furthermore, the information of some confounders like anthropometric factors, dietary pattern, nutritional status, lifestyle, smoking, alcohol drinking, family history, and genetic parameters was not available. Because only approximately 9% of the enrolled patients were pioglitazone users (Table 1), the models evaluating the dementia risk in subgroups of patients with pioglitazone use had low numbers of incident cases (models III and V of Table 3); therefore, the impact of these models might not be sufficient.
In conclusion, the present study finds a potential benefit of acarbose in reducing the risk of dementia in Taiwanese patients with type 2 diabetes mellitus. This benefit is especially significant in female patients, in non-users of metformin, and in patients who are treated with a combination of acarbose, metformin, and pioglitazone.
Conflicts of interest
The author declares no conflicts of interest.
Acknowledgments
The study is based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health and managed by National Health Research Institutes. The interpretation and conclusions contained herein do not represent those of Bureau of National Health Insurance, Department of Health or National Health Research Institutes. The study was supported by the Ministry of Science and Technology (MOST 107-2221-E-002-129-MY3) of Taiwan. The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
The 20-year voyage aboard the Journal of Alzheimer's Disease: Docking at 'Type 3 Diabetes', environmental/exposure factors, pathogenic mechanisms, and potential treatments
RadSK, AryaA, KarimianH, MadhavanP, RizwanF, KoshyS, et al. (2018).
Mechanism involved in insulin resistance via accumulation of β-amyloid and neurofibrillary tangles: link between type 2 diabetes and Alzheimer's disease
Long-term acarbose administration alleviating the impairment of spatial learning and memory in the SAMP8 mice was associated with alleviated reduction of insulin system and acetylated H4K8
Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies
Pharmacokinetics of acarbose. Part II: Distribution to and elimination from tissues and organs following single or repeated administration of [14C] acarbose to rats and dogs
HolmanRR, ColemanRL, ChanJCN, ChiassonJL, FengH, GeJ, et al. (2017).
Effects of acarbose on cardiovascular and diabetes outcomes in patients with coronary heart disease and impaired glucose tolerance (ACE): a randomised, double-blind, placebo-controlled trial
Problem of immortal time bias in cohort studies: example using statins for preventing progression of diabetes
. BMJ, 340: b5087.
Blood-brain barrier disturbances in diabetes-associated dementia: Therapeutic potential for cannabinoids
2
2019
... Dementia can either have a vascular etiology or occur because of a neurodegenerative disease such as Alzheimer’s disease (AD). Diabetes patients have a significantly 5-fold increased risk of dementia [1]. The close association between type 2 diabetes mellitus and AD and their potential common pathophysiological changes of impaired insulin expression and insulin resistance led to the coining of the term “type 3 diabetes” for AD [2]. The increased risk of dementia in diabetes patients may be due to the increased incidence of atherosclerosis, blood-brain barrier disturbances, and neurodegeneration associated with diabetes mellitus. The pathophysiological changes may include insulin resistance, increased deposition of advanced glycation end products, dysregulation of lipid metabolism, and augmented inflammation and oxidative stress [1,3]. Studies also suggest that postprandial glucose and glucose variability may increase the risk of cognitive dysfunction and dementia [4,5]. ...
... ]. The increased risk of dementia in diabetes patients may be due to the increased incidence of atherosclerosis, blood-brain barrier disturbances, and neurodegeneration associated with diabetes mellitus. The pathophysiological changes may include insulin resistance, increased deposition of advanced glycation end products, dysregulation of lipid metabolism, and augmented inflammation and oxidative stress [1,3]. Studies also suggest that postprandial glucose and glucose variability may increase the risk of cognitive dysfunction and dementia [4,5]. ...
The 20-year voyage aboard the Journal of Alzheimer's Disease: Docking at 'Type 3 Diabetes', environmental/exposure factors, pathogenic mechanisms, and potential treatments
3
2018
... Dementia can either have a vascular etiology or occur because of a neurodegenerative disease such as Alzheimer’s disease (AD). Diabetes patients have a significantly 5-fold increased risk of dementia [1]. The close association between type 2 diabetes mellitus and AD and their potential common pathophysiological changes of impaired insulin expression and insulin resistance led to the coining of the term “type 3 diabetes” for AD [2]. The increased risk of dementia in diabetes patients may be due to the increased incidence of atherosclerosis, blood-brain barrier disturbances, and neurodegeneration associated with diabetes mellitus. The pathophysiological changes may include insulin resistance, increased deposition of advanced glycation end products, dysregulation of lipid metabolism, and augmented inflammation and oxidative stress [1,3]. Studies also suggest that postprandial glucose and glucose variability may increase the risk of cognitive dysfunction and dementia [4,5]. ...
... Major brain pathological changes of AD include deposition of amyloid beta (Aβ) and hyper-phosphorylation of tau protein [2]. Aβ is formed by the cleaving of the amyloid precursor protein by secretases [6], and insulin resistance in the brain may aggravate the accumulation of Aβ [7]. Additionally, AD is characterized by neurodegeneration with damage in cholinergic neurons, resulting in reduced release of acetylcholine neurotransmitters [8]. Acetylcholinesterase and butyryl-cholinesterase are serine hydrolases that are responsible for the catalytic hydrolysis of acetylcholine and they play an important role in the aggregation of Aβ [9]. Therefore, cholinesterase inhibitors are the main drugs currently approved for AD treatment [8,10]. ...
... Theoretically, antidiabetic drugs that improve insulin resistance in the brain can potentially prevent AD or dementia [2]. As shown in our previous observational studies, two antidiabetic drugs, specifically metformin [11] and pioglitazone [12], that improve insulin resistance, show a reduced risk of dementia in a dose-response pattern in patients with type 2 diabetes mellitus. ...
Link between type 2 diabetes and Alzheimer's disease: from epidemiology to mechanism and treatment
1
2015
... Dementia can either have a vascular etiology or occur because of a neurodegenerative disease such as Alzheimer’s disease (AD). Diabetes patients have a significantly 5-fold increased risk of dementia [1]. The close association between type 2 diabetes mellitus and AD and their potential common pathophysiological changes of impaired insulin expression and insulin resistance led to the coining of the term “type 3 diabetes” for AD [2]. The increased risk of dementia in diabetes patients may be due to the increased incidence of atherosclerosis, blood-brain barrier disturbances, and neurodegeneration associated with diabetes mellitus. The pathophysiological changes may include insulin resistance, increased deposition of advanced glycation end products, dysregulation of lipid metabolism, and augmented inflammation and oxidative stress [1,3]. Studies also suggest that postprandial glucose and glucose variability may increase the risk of cognitive dysfunction and dementia [4,5]. ...
Postprandial plasma glucose excursions and cognitive functioning in aged type 2 diabetics
1
2006
... Dementia can either have a vascular etiology or occur because of a neurodegenerative disease such as Alzheimer’s disease (AD). Diabetes patients have a significantly 5-fold increased risk of dementia [1]. The close association between type 2 diabetes mellitus and AD and their potential common pathophysiological changes of impaired insulin expression and insulin resistance led to the coining of the term “type 3 diabetes” for AD [2]. The increased risk of dementia in diabetes patients may be due to the increased incidence of atherosclerosis, blood-brain barrier disturbances, and neurodegeneration associated with diabetes mellitus. The pathophysiological changes may include insulin resistance, increased deposition of advanced glycation end products, dysregulation of lipid metabolism, and augmented inflammation and oxidative stress [1,3]. Studies also suggest that postprandial glucose and glucose variability may increase the risk of cognitive dysfunction and dementia [4,5]. ...
Relationships between daily acute glucose fluctuations and cognitive performance among aged type 2 diabetic patients
1
2010
... Dementia can either have a vascular etiology or occur because of a neurodegenerative disease such as Alzheimer’s disease (AD). Diabetes patients have a significantly 5-fold increased risk of dementia [1]. The close association between type 2 diabetes mellitus and AD and their potential common pathophysiological changes of impaired insulin expression and insulin resistance led to the coining of the term “type 3 diabetes” for AD [2]. The increased risk of dementia in diabetes patients may be due to the increased incidence of atherosclerosis, blood-brain barrier disturbances, and neurodegeneration associated with diabetes mellitus. The pathophysiological changes may include insulin resistance, increased deposition of advanced glycation end products, dysregulation of lipid metabolism, and augmented inflammation and oxidative stress [1,3]. Studies also suggest that postprandial glucose and glucose variability may increase the risk of cognitive dysfunction and dementia [4,5]. ...
η-Secretase processing of APP inhibits neuronal activity in the hippocampus
1
2015
... Major brain pathological changes of AD include deposition of amyloid beta (Aβ) and hyper-phosphorylation of tau protein [2]. Aβ is formed by the cleaving of the amyloid precursor protein by secretases [6], and insulin resistance in the brain may aggravate the accumulation of Aβ [7]. Additionally, AD is characterized by neurodegeneration with damage in cholinergic neurons, resulting in reduced release of acetylcholine neurotransmitters [8]. Acetylcholinesterase and butyryl-cholinesterase are serine hydrolases that are responsible for the catalytic hydrolysis of acetylcholine and they play an important role in the aggregation of Aβ [9]. Therefore, cholinesterase inhibitors are the main drugs currently approved for AD treatment [8,10]. ...
Mechanism involved in insulin resistance via accumulation of β-amyloid and neurofibrillary tangles: link between type 2 diabetes and Alzheimer's disease
1
2018
... Major brain pathological changes of AD include deposition of amyloid beta (Aβ) and hyper-phosphorylation of tau protein [2]. Aβ is formed by the cleaving of the amyloid precursor protein by secretases [6], and insulin resistance in the brain may aggravate the accumulation of Aβ [7]. Additionally, AD is characterized by neurodegeneration with damage in cholinergic neurons, resulting in reduced release of acetylcholine neurotransmitters [8]. Acetylcholinesterase and butyryl-cholinesterase are serine hydrolases that are responsible for the catalytic hydrolysis of acetylcholine and they play an important role in the aggregation of Aβ [9]. Therefore, cholinesterase inhibitors are the main drugs currently approved for AD treatment [8,10]. ...
Target enzyme in Alzheimer's disease: Acetylcholinesterase inhibitors
2
2019
... Major brain pathological changes of AD include deposition of amyloid beta (Aβ) and hyper-phosphorylation of tau protein [2]. Aβ is formed by the cleaving of the amyloid precursor protein by secretases [6], and insulin resistance in the brain may aggravate the accumulation of Aβ [7]. Additionally, AD is characterized by neurodegeneration with damage in cholinergic neurons, resulting in reduced release of acetylcholine neurotransmitters [8]. Acetylcholinesterase and butyryl-cholinesterase are serine hydrolases that are responsible for the catalytic hydrolysis of acetylcholine and they play an important role in the aggregation of Aβ [9]. Therefore, cholinesterase inhibitors are the main drugs currently approved for AD treatment [8,10]. ...
... ]. Therefore, cholinesterase inhibitors are the main drugs currently approved for AD treatment [8,10]. ...
Current perspectives on pharmacotherapy of Alzheimer's disease
1
2011
... Major brain pathological changes of AD include deposition of amyloid beta (Aβ) and hyper-phosphorylation of tau protein [2]. Aβ is formed by the cleaving of the amyloid precursor protein by secretases [6], and insulin resistance in the brain may aggravate the accumulation of Aβ [7]. Additionally, AD is characterized by neurodegeneration with damage in cholinergic neurons, resulting in reduced release of acetylcholine neurotransmitters [8]. Acetylcholinesterase and butyryl-cholinesterase are serine hydrolases that are responsible for the catalytic hydrolysis of acetylcholine and they play an important role in the aggregation of Aβ [9]. Therefore, cholinesterase inhibitors are the main drugs currently approved for AD treatment [8,10]. ...
Present algorithms and future treatments for Alzheimer's disease
1
2019
... Major brain pathological changes of AD include deposition of amyloid beta (Aβ) and hyper-phosphorylation of tau protein [2]. Aβ is formed by the cleaving of the amyloid precursor protein by secretases [6], and insulin resistance in the brain may aggravate the accumulation of Aβ [7]. Additionally, AD is characterized by neurodegeneration with damage in cholinergic neurons, resulting in reduced release of acetylcholine neurotransmitters [8]. Acetylcholinesterase and butyryl-cholinesterase are serine hydrolases that are responsible for the catalytic hydrolysis of acetylcholine and they play an important role in the aggregation of Aβ [9]. Therefore, cholinesterase inhibitors are the main drugs currently approved for AD treatment [8,10]. ...
Metformin and the risk of dementia in type 2 diabetes patients
6
2019
... Theoretically, antidiabetic drugs that improve insulin resistance in the brain can potentially prevent AD or dementia [2]. As shown in our previous observational studies, two antidiabetic drugs, specifically metformin [11] and pioglitazone [12], that improve insulin resistance, show a reduced risk of dementia in a dose-response pattern in patients with type 2 diabetes mellitus. ...
... The cumulative duration of acarbose therapy in years was calculated from the database. Potential confounders included the following categories: demographic data, major comorbidities associated with diabetes mellitus, diabetes-related complications, potential risk factors for cancer, potential factors that may affect the prescription of acarbose, antidiabetic drugs, and medications commonly used in diabetes patients. Demographic data included age, sex, diabetes duration, occupation, and living region (classified as Taipei, Northern, Central, Southern, and Kao-Ping/Eastern). Occupation was classified as class I (civil servants, teachers, government employees or private businesses, professionals, and technicians), class II (people without a specific employer, self-employed people, or seamen), class III (farmers or fishermen) and class IV (low-income families supported by social welfare, or veterans). The ICD-9-CM codes for potential confounders categorized as major comorbidities associated with diabetes mellitus (hypertension, dyslipi-demia, and obesity), diabetes-related complications (nephropathy, eye disease, ischemic heart disease, and peripheral arterial disease), potential risk factors for cancer (chronic obstructive pulmonary disease, tobacco abuse, and alcohol-related diagnoses), and potential factors that may affect the prescription of acarbose (gallstone, diseases of the digestive system, Helicobacter Pylori infection, and/or Helicobacter Pylori eradication therapies, hepatitis B virus infection, hepatitis C virus infection, liver cirrhosis, and other chronic non-alcoholic liver diseases) can be found in previously published papers [11,12,22]. Antidiabetic drugs included insulin, sulfonylurea, metformin, meglitinide, rosiglitazone, and pioglitazone. Commonly used medications in diabetes patients included angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, calcium channel blockers, statins, fibrates, and aspirin. ...
... Because previous animal studies showed that acarbose may exert a better anti-aging effect in male mice than in female mice [24] and the use of either metformin [11] or pioglitazone [12] may reduce the risk of dementia, the incidence density of dementia was calculated for ever users and never users of acarbose in all patients and in subgroups of men, women, patients with metformin use, patients without metformin use, patients with pioglitazone use and patients without pioglitazone use, respectively, and for different subgroups of combinations of the use of acarbose, metformin and pioglitazone. The numerator was the number of newly diagnosed cases of dementia patients identified during follow-up and the denominator was the follow-up duration in person-years. Follow-up started on January 1, 2007, and ended on December 31, 2011, at the time of a new diagnosis of dementia, or on the date of death or the last reimbursement record, whichever occurred first. ...
... As shown in our previous studies, metformin [11] and pioglitazone [12] improve insulin resistance and are associated with a lower risk of dementia. This study provided information to support the potential role of insulin resistance in dementia in patients with type 2 diabetes mellitus because acarbose may also reduce insulin resistance, though to a lesser extent. However, unlike metformin and pioglitazone that may pass through the blood-brain barrier [11,12], acarbose or its metabolites do not cross the blood-brain barrier [24]. Therefore, acarbose may not act directly on the central nervous system. Acarbose is especially useful for reducing postprandial glucose and it is less likely to cause hypoglycemia [13,15]. Therefore, the reduced oxidative stress because of reduced glucose variability in patients treated with acarbose may contribute to a reduced risk of dementia. The improvement of lipid profile, inhibition of platelet activation, and the reduction of inflammation associated with acarbose use [13,15] may also partly explain the reduced risk of dementia associated with acarbose. ...
... ] improve insulin resistance and are associated with a lower risk of dementia. This study provided information to support the potential role of insulin resistance in dementia in patients with type 2 diabetes mellitus because acarbose may also reduce insulin resistance, though to a lesser extent. However, unlike metformin and pioglitazone that may pass through the blood-brain barrier [11,12], acarbose or its metabolites do not cross the blood-brain barrier [24]. Therefore, acarbose may not act directly on the central nervous system. Acarbose is especially useful for reducing postprandial glucose and it is less likely to cause hypoglycemia [13,15]. Therefore, the reduced oxidative stress because of reduced glucose variability in patients treated with acarbose may contribute to a reduced risk of dementia. The improvement of lipid profile, inhibition of platelet activation, and the reduction of inflammation associated with acarbose use [13,15] may also partly explain the reduced risk of dementia associated with acarbose. ...
... The subgroup analyses suggested that the beneficial effect of acarbose on dementia was mainly observed in female patients (Table 2) and in non-users of metformin (model II of Table 3). Metformin is protective against dementia per se [11] and it is always used as a first-line treatment for type 2 diabetes mellitus. Therefore, patients who used both metformin and acarbose in the study might have been benefited from the protection against dementia by metformin and the benefit of acarbose might not be additive to the effect of metformin. It is worthy to note that the beneficial effect of metformin on dementia could also be demonstrated in the present study by comparing the incidence rates of dementia in patients who were using metformin versus those who were not using metformin in never users of acarbose (332.42 versus 523.07 per 100,000 person-years) and in ever users of acarbose (309.78 versus 380.13 per 100,000 person-years), respectively (Models I and II of Table 3). Similarly, female patients seemed to suffer from a higher incidence of dementia than male patients in acarbose never users and ever users, respectively (Table 2). ...
Pioglitazone reduces dementia risk in patients with type 2 diabetes mellitus: a retrospective cohort analysis
5
2018
... Theoretically, antidiabetic drugs that improve insulin resistance in the brain can potentially prevent AD or dementia [2]. As shown in our previous observational studies, two antidiabetic drugs, specifically metformin [11] and pioglitazone [12], that improve insulin resistance, show a reduced risk of dementia in a dose-response pattern in patients with type 2 diabetes mellitus. ...
... The cumulative duration of acarbose therapy in years was calculated from the database. Potential confounders included the following categories: demographic data, major comorbidities associated with diabetes mellitus, diabetes-related complications, potential risk factors for cancer, potential factors that may affect the prescription of acarbose, antidiabetic drugs, and medications commonly used in diabetes patients. Demographic data included age, sex, diabetes duration, occupation, and living region (classified as Taipei, Northern, Central, Southern, and Kao-Ping/Eastern). Occupation was classified as class I (civil servants, teachers, government employees or private businesses, professionals, and technicians), class II (people without a specific employer, self-employed people, or seamen), class III (farmers or fishermen) and class IV (low-income families supported by social welfare, or veterans). The ICD-9-CM codes for potential confounders categorized as major comorbidities associated with diabetes mellitus (hypertension, dyslipi-demia, and obesity), diabetes-related complications (nephropathy, eye disease, ischemic heart disease, and peripheral arterial disease), potential risk factors for cancer (chronic obstructive pulmonary disease, tobacco abuse, and alcohol-related diagnoses), and potential factors that may affect the prescription of acarbose (gallstone, diseases of the digestive system, Helicobacter Pylori infection, and/or Helicobacter Pylori eradication therapies, hepatitis B virus infection, hepatitis C virus infection, liver cirrhosis, and other chronic non-alcoholic liver diseases) can be found in previously published papers [11,12,22]. Antidiabetic drugs included insulin, sulfonylurea, metformin, meglitinide, rosiglitazone, and pioglitazone. Commonly used medications in diabetes patients included angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, calcium channel blockers, statins, fibrates, and aspirin. ...
... Because previous animal studies showed that acarbose may exert a better anti-aging effect in male mice than in female mice [24] and the use of either metformin [11] or pioglitazone [12] may reduce the risk of dementia, the incidence density of dementia was calculated for ever users and never users of acarbose in all patients and in subgroups of men, women, patients with metformin use, patients without metformin use, patients with pioglitazone use and patients without pioglitazone use, respectively, and for different subgroups of combinations of the use of acarbose, metformin and pioglitazone. The numerator was the number of newly diagnosed cases of dementia patients identified during follow-up and the denominator was the follow-up duration in person-years. Follow-up started on January 1, 2007, and ended on December 31, 2011, at the time of a new diagnosis of dementia, or on the date of death or the last reimbursement record, whichever occurred first. ...
... As shown in our previous studies, metformin [11] and pioglitazone [12] improve insulin resistance and are associated with a lower risk of dementia. This study provided information to support the potential role of insulin resistance in dementia in patients with type 2 diabetes mellitus because acarbose may also reduce insulin resistance, though to a lesser extent. However, unlike metformin and pioglitazone that may pass through the blood-brain barrier [11,12], acarbose or its metabolites do not cross the blood-brain barrier [24]. Therefore, acarbose may not act directly on the central nervous system. Acarbose is especially useful for reducing postprandial glucose and it is less likely to cause hypoglycemia [13,15]. Therefore, the reduced oxidative stress because of reduced glucose variability in patients treated with acarbose may contribute to a reduced risk of dementia. The improvement of lipid profile, inhibition of platelet activation, and the reduction of inflammation associated with acarbose use [13,15] may also partly explain the reduced risk of dementia associated with acarbose. ...
... ,12], acarbose or its metabolites do not cross the blood-brain barrier [24]. Therefore, acarbose may not act directly on the central nervous system. Acarbose is especially useful for reducing postprandial glucose and it is less likely to cause hypoglycemia [13,15]. Therefore, the reduced oxidative stress because of reduced glucose variability in patients treated with acarbose may contribute to a reduced risk of dementia. The improvement of lipid profile, inhibition of platelet activation, and the reduction of inflammation associated with acarbose use [13,15] may also partly explain the reduced risk of dementia associated with acarbose. ...
On the potential of acarbose to reduce cardiovascular disease
4
2014
... Acarbose, an alpha-glucosidase inhibitor that inhibits the digestion of carbohydrate in the intestine, is commonly used to treat diabetes in Asian populations, probably because of its glucose lowering effect for patients who consume Asian diets that have a high content of carbohydrate [13,14]. Acarbose has the following benefits that may contribute to a reduction of dementia risk: lowering postprandial glucose with a lower risk of hypoglycemia, improving insulin resistance, improving lipid profile, enhancing the release of glucagon-like peptide-1, inhibiting platelet activation, exerting anti-inflammatory effect, and reducing oxidative stress [13,15]. Indeed, novel drugs that may exert inhibitory effects on alpha glucosidase and cholinesterase are being developed for the treatment of both type 2 diabetes mellitus and AD [16]. ...
... ]. Acarbose has the following benefits that may contribute to a reduction of dementia risk: lowering postprandial glucose with a lower risk of hypoglycemia, improving insulin resistance, improving lipid profile, enhancing the release of glucagon-like peptide-1, inhibiting platelet activation, exerting anti-inflammatory effect, and reducing oxidative stress [13,15]. Indeed, novel drugs that may exert inhibitory effects on alpha glucosidase and cholinesterase are being developed for the treatment of both type 2 diabetes mellitus and AD [16]. ...
... As shown in our previous studies, metformin [11] and pioglitazone [12] improve insulin resistance and are associated with a lower risk of dementia. This study provided information to support the potential role of insulin resistance in dementia in patients with type 2 diabetes mellitus because acarbose may also reduce insulin resistance, though to a lesser extent. However, unlike metformin and pioglitazone that may pass through the blood-brain barrier [11,12], acarbose or its metabolites do not cross the blood-brain barrier [24]. Therefore, acarbose may not act directly on the central nervous system. Acarbose is especially useful for reducing postprandial glucose and it is less likely to cause hypoglycemia [13,15]. Therefore, the reduced oxidative stress because of reduced glucose variability in patients treated with acarbose may contribute to a reduced risk of dementia. The improvement of lipid profile, inhibition of platelet activation, and the reduction of inflammation associated with acarbose use [13,15] may also partly explain the reduced risk of dementia associated with acarbose. ...
... ]. Therefore, the reduced oxidative stress because of reduced glucose variability in patients treated with acarbose may contribute to a reduced risk of dementia. The improvement of lipid profile, inhibition of platelet activation, and the reduction of inflammation associated with acarbose use [13,15] may also partly explain the reduced risk of dementia associated with acarbose. ...
Safety and efficacy of acarbose in the treatment of diabetes in Chinese patients
1
2014
... Acarbose, an alpha-glucosidase inhibitor that inhibits the digestion of carbohydrate in the intestine, is commonly used to treat diabetes in Asian populations, probably because of its glucose lowering effect for patients who consume Asian diets that have a high content of carbohydrate [13,14]. Acarbose has the following benefits that may contribute to a reduction of dementia risk: lowering postprandial glucose with a lower risk of hypoglycemia, improving insulin resistance, improving lipid profile, enhancing the release of glucagon-like peptide-1, inhibiting platelet activation, exerting anti-inflammatory effect, and reducing oxidative stress [13,15]. Indeed, novel drugs that may exert inhibitory effects on alpha glucosidase and cholinesterase are being developed for the treatment of both type 2 diabetes mellitus and AD [16]. ...
Acarbose: safe and effective for lowering postprandial hyperglycaemia and improving cardiovascular outcomes
3
2015
... Acarbose, an alpha-glucosidase inhibitor that inhibits the digestion of carbohydrate in the intestine, is commonly used to treat diabetes in Asian populations, probably because of its glucose lowering effect for patients who consume Asian diets that have a high content of carbohydrate [13,14]. Acarbose has the following benefits that may contribute to a reduction of dementia risk: lowering postprandial glucose with a lower risk of hypoglycemia, improving insulin resistance, improving lipid profile, enhancing the release of glucagon-like peptide-1, inhibiting platelet activation, exerting anti-inflammatory effect, and reducing oxidative stress [13,15]. Indeed, novel drugs that may exert inhibitory effects on alpha glucosidase and cholinesterase are being developed for the treatment of both type 2 diabetes mellitus and AD [16]. ...
... As shown in our previous studies, metformin [11] and pioglitazone [12] improve insulin resistance and are associated with a lower risk of dementia. This study provided information to support the potential role of insulin resistance in dementia in patients with type 2 diabetes mellitus because acarbose may also reduce insulin resistance, though to a lesser extent. However, unlike metformin and pioglitazone that may pass through the blood-brain barrier [11,12], acarbose or its metabolites do not cross the blood-brain barrier [24]. Therefore, acarbose may not act directly on the central nervous system. Acarbose is especially useful for reducing postprandial glucose and it is less likely to cause hypoglycemia [13,15]. Therefore, the reduced oxidative stress because of reduced glucose variability in patients treated with acarbose may contribute to a reduced risk of dementia. The improvement of lipid profile, inhibition of platelet activation, and the reduction of inflammation associated with acarbose use [13,15] may also partly explain the reduced risk of dementia associated with acarbose. ...
... ,15] may also partly explain the reduced risk of dementia associated with acarbose. ...
2-Furoic piperazide derivatives as promising drug candidates of type 2 diabetes and Alzheimer's diseases: In vitro and in silico studies
2
2018
... Acarbose, an alpha-glucosidase inhibitor that inhibits the digestion of carbohydrate in the intestine, is commonly used to treat diabetes in Asian populations, probably because of its glucose lowering effect for patients who consume Asian diets that have a high content of carbohydrate [13,14]. Acarbose has the following benefits that may contribute to a reduction of dementia risk: lowering postprandial glucose with a lower risk of hypoglycemia, improving insulin resistance, improving lipid profile, enhancing the release of glucagon-like peptide-1, inhibiting platelet activation, exerting anti-inflammatory effect, and reducing oxidative stress [13,15]. Indeed, novel drugs that may exert inhibitory effects on alpha glucosidase and cholinesterase are being developed for the treatment of both type 2 diabetes mellitus and AD [16]. ...
... In recent decades, there has been a dramatic increase in diabetes worldwide, and millions of patients are using antidiabetic drugs. This study may have some clinical and research significance because acarbose remains an important oral antidiabetic drug, especially in Asian populations. Although no definite beneficial effects on cardiovascular disease were observed with acarbose treatment in a clinical trial conducted in the Chinese population in China [25], the potential benefit of acarbose on dementia in specific subgroups of patients, i.e., in female patients (Table 2), in non-users of metformin (model II of Table 3) and in combination with metformin and pioglitazone (group 7 in model V of Table 3), provides rationale for repositioning acarbose in the treatment of Chinese patients with type 2 diabetes mellitus. At least, based on current evidence, acarbose may be considered in patients who consume large amounts of carbohydrate and it can be used as a substitute for metformin in patients who are at risk of dementia but contraindicated for metformin use or who cannot tolerate the side effects of metformin, especially in female patients. A combination of acarbose, metformin, and pioglitazone may be a good choice in some patients who require greater control of blood glucose. Such a combination theoretically provides a better glycemic control without the risk of hypoglycemia and with a much more reduced insulin resistance. The findings of the present study also provide rationale for the development of novel drugs that can pass through the blood-brain barrier and exert dual inhibitory effects on alpha glucosidase and cholinesterase for targeting the treatment of both type 2 diabetes mellitus and AD [16]. ...
Long-term acarbose administration alleviating the impairment of spatial learning and memory in the SAMP8 mice was associated with alleviated reduction of insulin system and acetylated H4K8
1
2015
... A recent animal study suggested that acarbose has a protective effect on the decline of cognitive function, including spatial learning and memory, in SAMP8 mice [17]. However, a recent small scale randomized clinical trial conducted in patients with non-dementia vascular cognitive impairment and abnormal glucose metabolism showed an improvement in cognitive function only in patients assigned to metformin and donepezil (n = 50) for one year but not in those assigned to acarbose and donepezil (n = 50) [18]. Whether prolonged use of acarbose in diabetes treatment might exert a potential benefit for dementia has not been investigated. The present study investigated dementia risk in patients with type 2 diabetes mellitus who had been treated with acarbose and those who had never been treated with acarbose in the Chinese population in Taiwan by using the reimbursement database of the National Health Insurance (NHI). ...
Evaluation of metformin on cognitive improvement in patients with non-dementia vascular cognitive impairment and abnormal glucose metabolism
1
2018
... A recent animal study suggested that acarbose has a protective effect on the decline of cognitive function, including spatial learning and memory, in SAMP8 mice [17]. However, a recent small scale randomized clinical trial conducted in patients with non-dementia vascular cognitive impairment and abnormal glucose metabolism showed an improvement in cognitive function only in patients assigned to metformin and donepezil (n = 50) for one year but not in those assigned to acarbose and donepezil (n = 50) [18]. Whether prolonged use of acarbose in diabetes treatment might exert a potential benefit for dementia has not been investigated. The present study investigated dementia risk in patients with type 2 diabetes mellitus who had been treated with acarbose and those who had never been treated with acarbose in the Chinese population in Taiwan by using the reimbursement database of the National Health Insurance (NHI). ...
Metformin and lung cancer risk in patients with type 2 diabetes mellitus
1
2017
... The approval number for the present study was 99274 by the National Health Research Institutes and the database was described in detail in previous papers [19,20]. Throughout the study period, diabetes was coded 250.XX according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) and dementia was coded as abridged codes of A210 or A222, or as ICD-9-CM codes of 290.0, 290.1, 290.2, 290.4, 294.1, 331.0-331.2, or 331.7-331.9. ...
Metformin is associated with a lower risk of colorectal cancer in Taiwanese patients with type 2 diabetes: a retrospective cohort analysis
1
2017
... The approval number for the present study was 99274 by the National Health Research Institutes and the database was described in detail in previous papers [19,20]. Throughout the study period, diabetes was coded 250.XX according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) and dementia was coded as abridged codes of A210 or A222, or as ICD-9-CM codes of 290.0, 290.1, 290.2, 290.4, 294.1, 331.0-331.2, or 331.7-331.9. ...
Performing a 1:N case-control match on propensity score
1
2019
... The procedures used to create a cohort of 1:1 matched pair of ever users and never users of acarbose are shown in Figure 1. At first, 446,105 patients who had new-onset diabetes mellitus from 1999 to 2006 and who had been prescribed antidiabetic drugs two or more times were identified from the outpatient clinics. Patients diagnosed with diabetes mellitus between 1996 and 1998 were excluded to ensure that only patients with new-onset diabetes were included in the study. The following patients were then excluded: 1) patients who had been diagnosed with dementia and/or died before January 1, 2007 (n = 25,565); 2) patients who were initiated with acarbose after January 1, 2007 (n = 81,689); 3) patients with type 1 diabetes mellitus (n = 2263); 4) patients with missing data (n = 493); 5) patients who had used acarbose for <180 days (n = 15,336); 6) patients with a diagnosis of any cancer before entry (n = 35,251, cancer patients were excluded because they might have shortened lifespans which might have distorted follow-up time and dementia could be misdiagnosed from the clinical presentations of malignancy); 7) patients aged <25 years (n = 1192); 8) patients aged >75 years (n = 32,570); 9) patients with Parkinson’s disease before entry (n = 2718); 10) patients with head injury before entry (n = 3158); 11) patients with a diagnosis of hypoglycemia before entry (n = 2337); 12) patients with a history of stroke before entry (n = 43,178); and 13) patients with a follow-up duration < 180 days (n = 4675). Patients with Parkinson’s disease, head injury, hypoglycemia, and stroke were excluded because these diagnoses are important risk factors for dementia. As a result, 15,566 ever users and 180,114 never users of acarbose were identified (unmatched original cohort). A cohort of 1:1 matched pairs of 15,524 ever users and 15,524 never users (the matched cohort) was created by propensity score matching based on the Greedy 8→1 digit match algorithm [21]. Logistic regression was used to create the propensity score from all characteristics listed in Table 1 being treated as independent variables. ...
Metformin decreases risk of tuberculosis infection in type 2 diabetes patients
1
2018
... The cumulative duration of acarbose therapy in years was calculated from the database. Potential confounders included the following categories: demographic data, major comorbidities associated with diabetes mellitus, diabetes-related complications, potential risk factors for cancer, potential factors that may affect the prescription of acarbose, antidiabetic drugs, and medications commonly used in diabetes patients. Demographic data included age, sex, diabetes duration, occupation, and living region (classified as Taipei, Northern, Central, Southern, and Kao-Ping/Eastern). Occupation was classified as class I (civil servants, teachers, government employees or private businesses, professionals, and technicians), class II (people without a specific employer, self-employed people, or seamen), class III (farmers or fishermen) and class IV (low-income families supported by social welfare, or veterans). The ICD-9-CM codes for potential confounders categorized as major comorbidities associated with diabetes mellitus (hypertension, dyslipi-demia, and obesity), diabetes-related complications (nephropathy, eye disease, ischemic heart disease, and peripheral arterial disease), potential risk factors for cancer (chronic obstructive pulmonary disease, tobacco abuse, and alcohol-related diagnoses), and potential factors that may affect the prescription of acarbose (gallstone, diseases of the digestive system, Helicobacter Pylori infection, and/or Helicobacter Pylori eradication therapies, hepatitis B virus infection, hepatitis C virus infection, liver cirrhosis, and other chronic non-alcoholic liver diseases) can be found in previously published papers [11,12,22]. Antidiabetic drugs included insulin, sulfonylurea, metformin, meglitinide, rosiglitazone, and pioglitazone. Commonly used medications in diabetes patients included angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, calcium channel blockers, statins, fibrates, and aspirin. ...
Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies
1
2015
... Student’s t test was used to compare the differences of age and diabetes duration between never and ever users and the Chi-square test was used for other variables. According to Austin and Stuart, a standardized difference was calculated for each covariate and a cutoff value of >10% was used as an indicator of potential confounding from the variable [23]. ...
Acarbose, 17-α-estradiol, and nordihydroguaiaretic acid extend mouse lifespan preferentially in males
5
2014
... Because previous animal studies showed that acarbose may exert a better anti-aging effect in male mice than in female mice [24] and the use of either metformin [11] or pioglitazone [12] may reduce the risk of dementia, the incidence density of dementia was calculated for ever users and never users of acarbose in all patients and in subgroups of men, women, patients with metformin use, patients without metformin use, patients with pioglitazone use and patients without pioglitazone use, respectively, and for different subgroups of combinations of the use of acarbose, metformin and pioglitazone. The numerator was the number of newly diagnosed cases of dementia patients identified during follow-up and the denominator was the follow-up duration in person-years. Follow-up started on January 1, 2007, and ended on December 31, 2011, at the time of a new diagnosis of dementia, or on the date of death or the last reimbursement record, whichever occurred first. ...
... As shown in our previous studies, metformin [11] and pioglitazone [12] improve insulin resistance and are associated with a lower risk of dementia. This study provided information to support the potential role of insulin resistance in dementia in patients with type 2 diabetes mellitus because acarbose may also reduce insulin resistance, though to a lesser extent. However, unlike metformin and pioglitazone that may pass through the blood-brain barrier [11,12], acarbose or its metabolites do not cross the blood-brain barrier [24]. Therefore, acarbose may not act directly on the central nervous system. Acarbose is especially useful for reducing postprandial glucose and it is less likely to cause hypoglycemia [13,15]. Therefore, the reduced oxidative stress because of reduced glucose variability in patients treated with acarbose may contribute to a reduced risk of dementia. The improvement of lipid profile, inhibition of platelet activation, and the reduction of inflammation associated with acarbose use [13,15] may also partly explain the reduced risk of dementia associated with acarbose. ...
... The differential effects of acarbose on dementia risk in male and female patients are interesting. Previous animal studies also suggested differential effects of acarbose on lifespan prolongation in male and female mice [24]. While acarbose increased the median lifespan by 22% in male mice (P-value < 0.0001), it increased the lifespan in female mice by only 5% (P-value = 0.01) [24]. Although acarbose was beneficial in prolonging the lifespan in male mice [24], its benefit on dementia seemed to be more predominant in the female patients in the present study (Table 2). The reason for such a discrepancy between different sexes in terms of lifespan in mice and in terms of dementia in humans remains unknown. ...
... ]. While acarbose increased the median lifespan by 22% in male mice (P-value < 0.0001), it increased the lifespan in female mice by only 5% (P-value = 0.01) [24]. Although acarbose was beneficial in prolonging the lifespan in male mice [24], its benefit on dementia seemed to be more predominant in the female patients in the present study (Table 2). The reason for such a discrepancy between different sexes in terms of lifespan in mice and in terms of dementia in humans remains unknown. ...
... ]. Although acarbose was beneficial in prolonging the lifespan in male mice [24], its benefit on dementia seemed to be more predominant in the female patients in the present study (Table 2). The reason for such a discrepancy between different sexes in terms of lifespan in mice and in terms of dementia in humans remains unknown. ...
Pharmacokinetics of acarbose. Part II: Distribution to and elimination from tissues and organs following single or repeated administration of [14C] acarbose to rats and dogs
1
1989
... In recent decades, there has been a dramatic increase in diabetes worldwide, and millions of patients are using antidiabetic drugs. This study may have some clinical and research significance because acarbose remains an important oral antidiabetic drug, especially in Asian populations. Although no definite beneficial effects on cardiovascular disease were observed with acarbose treatment in a clinical trial conducted in the Chinese population in China [25], the potential benefit of acarbose on dementia in specific subgroups of patients, i.e., in female patients (Table 2), in non-users of metformin (model II of Table 3) and in combination with metformin and pioglitazone (group 7 in model V of Table 3), provides rationale for repositioning acarbose in the treatment of Chinese patients with type 2 diabetes mellitus. At least, based on current evidence, acarbose may be considered in patients who consume large amounts of carbohydrate and it can be used as a substitute for metformin in patients who are at risk of dementia but contraindicated for metformin use or who cannot tolerate the side effects of metformin, especially in female patients. A combination of acarbose, metformin, and pioglitazone may be a good choice in some patients who require greater control of blood glucose. Such a combination theoretically provides a better glycemic control without the risk of hypoglycemia and with a much more reduced insulin resistance. The findings of the present study also provide rationale for the development of novel drugs that can pass through the blood-brain barrier and exert dual inhibitory effects on alpha glucosidase and cholinesterase for targeting the treatment of both type 2 diabetes mellitus and AD [16]. ...
Effects of acarbose on cardiovascular and diabetes outcomes in patients with coronary heart disease and impaired glucose tolerance (ACE): a randomised, double-blind, placebo-controlled trial
2
2017
... Immortal time refers to the follow-up period when the outcome cannot occur. Therefore, immortal time bias can be introduced when the treatment status or follow-up time is inappropriately assigned [26]. In the present study, ambiguous diagnosis of diabetes was unlikely because only patients who had been prescribed antidiabetic drugs two or more times had been enrolled (Figure 1). Misclassification of treatment status was also unlikely in Taiwan because the NHI is a universal healthcare system and the information of all prescriptions was completely stored in computer files during the whole study period. Therefore, misdiagnosis of diabetes and misclassification of treatment status were well avoided. ...
... The follow-up time of the patients was also carefully considered to avoid the inclusion of immortal time. First, immortal time bias was avoided by excluding patients who had a short follow-up period of < 180 days (Figure 1). The immortal time between diabetes diagnosis and the start of the use of antidiabetic drugs had been avoided because patients were enrolled only when they started with the treatment of antidiabetic drugs and immortal time was actually not calculated in the person-years. The immortal time introduced during the waiting period between the prescription and the dispensing of medications after hospital discharge as described by Lévesque et al. [26] would not occur in Taiwan because all discharge medications can be obtained directly from the hospital when the patients are discharged. ...
Problem of immortal time bias in cohort studies: example using statins for preventing progression of diabetes
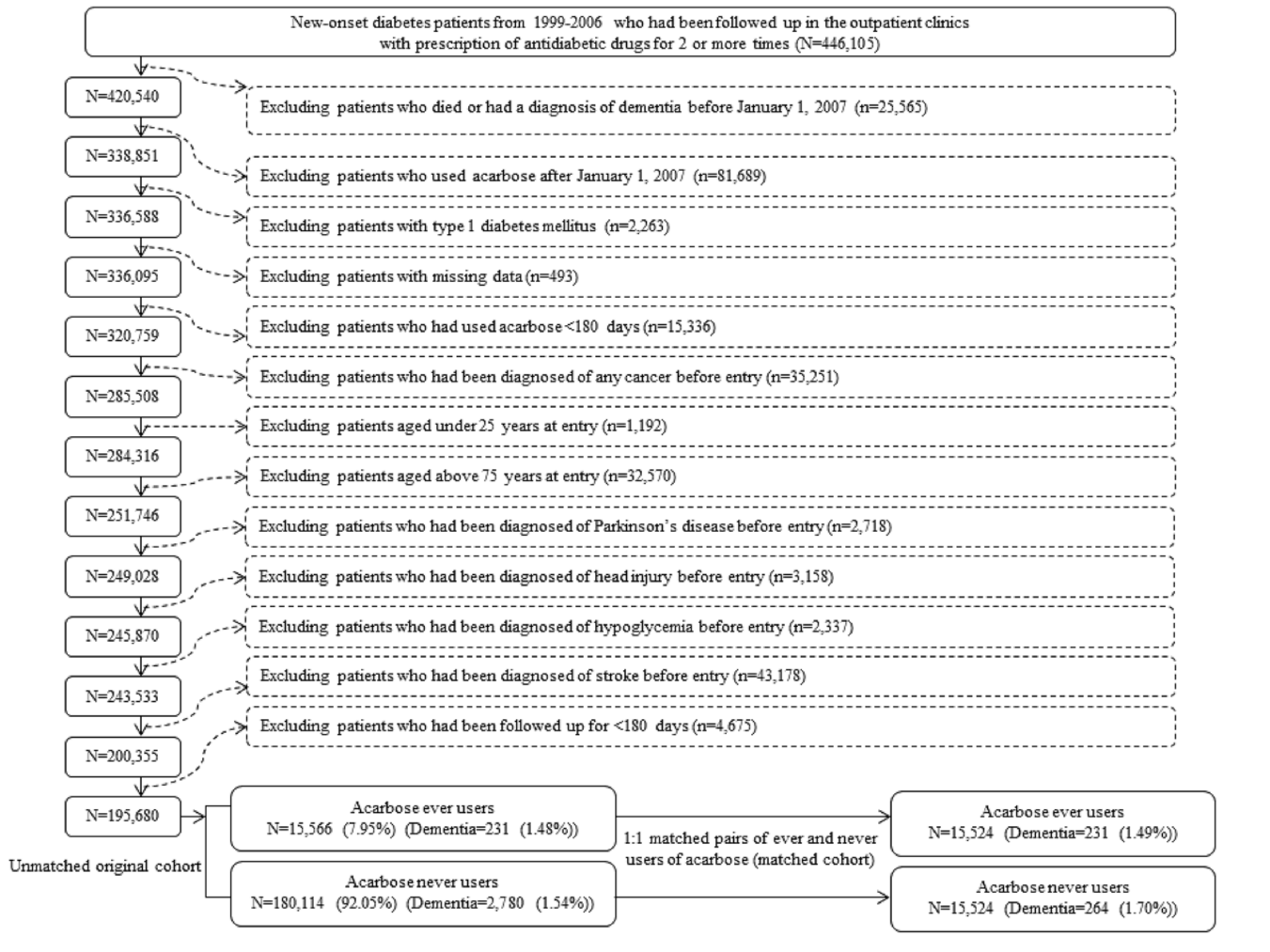
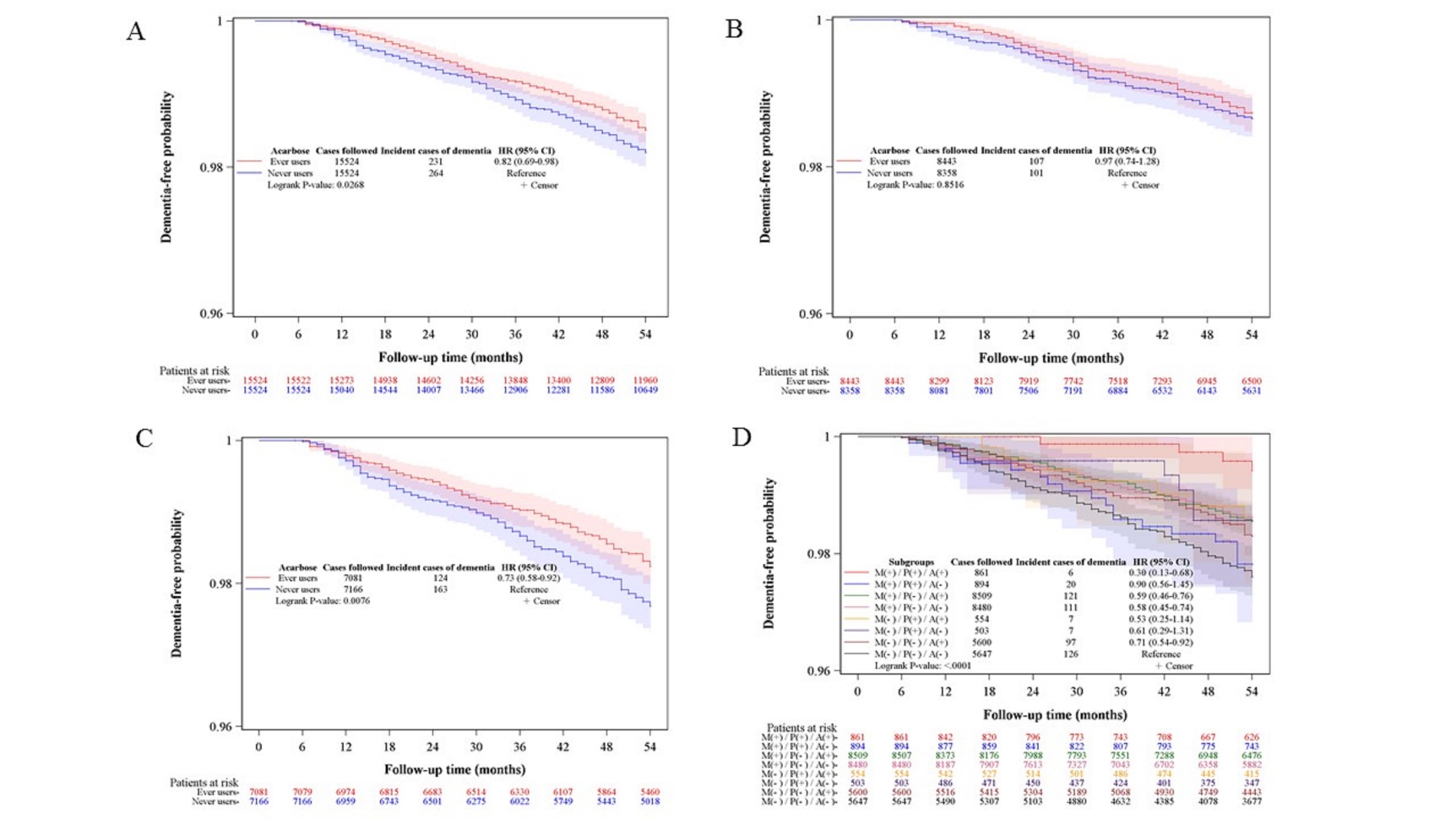
{kind=link}
{kind=link}
{kind=link}
{kind=link}



