COVID-19 in Elderly Adults: Clinical Features, Molecular Mechanisms, and Proposed Strategies
Yang Ya#, Zhao Yalei#, Zhang Fen, Zhang Lingjian, Li Lanjuan*
State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, National Clinical Research Center for Infectious Diseases, Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, The First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou, China.
通讯作者: Correspondence should be addressed to: Dr. Lanjuan Li, The First Affiliated Hospital, College of Medicine, Zhejiang University, 310003 Hangzhou, Zhejiang Province, China. E-mail: ljli@zju.edu.cn.Correspondence should be addressed to: Dr. Lanjuan Li, The First Affiliated Hospital, College of Medicine, Zhejiang University, 310003 Hangzhou, Zhejiang Province, China. E-mail: ljli@zju.edu.cn.
收稿日期:2020-07-5
修回日期: 2020-09-1
接受日期: 2020-09-3
网络出版日期: 2020-12-01
版权声明:
2020 this is an open access article distributed under the terms of the creative commons attribution license, which permits unrestricted use, distribution and reproduction in any medium provided that the original work is properly attributed.
作者简介:
These authors contrinuted equally to this work.
展开
Abstract
Coronavirus disease 2019 (COVID-19) is causing problems worldwide. Most people are susceptible to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), but elderly populations are more susceptible. Elevated susceptibility and death rates in elderly COVID-19 patients, especially those with age-related complications, are challenges for pandemic prevention and control. In this paper, we review the clinical features of elderly patients with COVID-19 and explore the related molecular mechanisms that are essential for the exploration of preventive and therapeutic strategies in the current pandemic. Furthermore, we analyze the feasibility of currently recommended potential novel methods against COVID-19 among elderly populations.
YangYa, ZhaoYalei, ZhangFen, ZhangLingjian, LiLanjuan. COVID-19 in Elderly Adults: Clinical Features, Molecular Mechanisms, and Proposed Strategies[J]. Aging and Disease, 2020, 11(6): 1481-1495 https://doi.org/10.14336/AD.2020.0903
Coronavirus disease 2019 (COVID-19) is an emerging respiratory infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which was first identified in mid-December 2019 in Wuhan, China. Currently, it has spread globally and been declared a pandemic by the World Health Organization (WHO). Up to August 18,2020, more than 767,000 deaths and 21,500,000 confirmed positive cases have been reported around the world. Accumulating evidence shows that age and underlying conditions of virus contacts are crucial factors influencing personal fate toward different clinical severities of COVID-19, ranging from asymptomatic, mild, and moderate to death [1, 2]. COVID-19 shows a considerably elevated mortality rate in patients with advanced age and pre-existing comorbidities [3]. Under the situation of global aging, the COVID-19 pandemic creates challenges for not only widespread public health but also biomedical and clinical aging research [4].
Clinical features of COVID-19 in elderly patients
New coronavirus-exposed populations are generally susceptible, but elderly people, especially those with underlying conditions normally considered to be aging-associated diseases (diabetes, hypertension, and cardiovascular and cerebrovascular diseases), exhibit increased susceptibility [5]. Moreover, the spread of SARS-CoV-2 as well as severe acute respiratory syndrome coronavirus (SARS-CoV) in 2003 made it clear that these aging patients are more likely to progress to severe disease and die more easily from these infections than younger people [6-8]. After analyzing the data for 1099 COVID-19 patients from 552 hospitals in China, Nanshan Zhong et al. found that patients with severe disease were older than those with nonsevere disease and that coexisting illness was more common among patients in the severe group[9]. In the United States, 80% of deaths have occurred in patients over the age of 65 years, and patients aged 85 years and over have a high proportion of severe outcomes, mirroring the experience in China [10]. According to a meta-analysis, serious aging-related chronic diseases(associated with a pathological role of cellular senescence), including hypertension, diabetes, chronic obstructive pulmonary disease (COPD), cardiovascular disease, and cerebrovascular disease, are independent risk factors associated with COVID-19 patients [11].
Similar to those in younger patients, fever, cough and sputum are the most common early symptoms in elderly patients. Elderly patients are more likely to have severe COVID-19 conditions, show lack of improvement, and die [12]. Analyzing a total of 56 COVID-19 patients, Liu et al. found that the pneumonia severity index (PSI) score of elderly patients was higher than that of young and middle-aged patients. The proportion of patients with PSI grades IV and V was significantly higher in elderly patients [13]. The incidence of the common fatal presentations of COVID-19 (including ARDS, shock, arrhythmia and acute cardiac injury) in elderly patients is higher than in young patients [12, 14, 15]. Wang et al. included patients with laboratory-confirmed COVID-19 and ascurtained the viral load by reverse transcriptase quantitative PCR (RT-qPCR). The results showed that older age was correlated with higher SARS-CoV-2 load [16]. Studies of SARS-CoV have shown that a high initial viral load is associated with death [17]. Accumulating evidence indicates that the SARS-CoV-2 viral load correlates with the risk of COVID-19 progression and poor prognosis [18, 19]. Thus, it is conceivable that the poor prognosis of elderly COVID-19 patients may be related to a higher viral load. However, the underlying mechanism requires further exploration.
Mechanism of COVID-19 in elderly patients
Senescent cells accumulate with age in vertebrates and promote aging mainly through the senescence-associated secretory phenotype (SASP) [20]. Data have shown that RNA viruses, such as influenza virus, display enhanced replication efficiency in senescent cells, which suggests that the accumulation of senescent cells in aging and age-related diseases may play a role in this phenomenon. However, the response to SARS-COV-2 that occurs in senescent cells is still poorly understood [8].
Angiotensin-converting enzyme 2 (ACE2) has been identified as areceptor for SARS-CoV-2, which directly interacts with COVID-19 spike(S) glycoproteins [21, 22]. During infection, the S protein is cleaved into S1 andS2 by the host transmembrane protease/serine subfamily member 2 (TMPRSS2)and protease furin [23].S1 directly binds to ACE2 and S2 plays a role in membrane fusion [24]. Zhou et al. analysed the expression of ACE2, together withTMPRSS2 and Furin by the method of single-cell RNA profiling combined with the protein information in different tissues. According to the rank list of candidate cells potentially vulnerable to SARS-CoV-2,the top targets were lung alveolar type 2 (AT2) cells and macrophages, followed by cardiomyocytes and adrenal gland stromal cells [25]. These findings were consistent with prominent lung symptoms, frequent heart damage and rare bowel symptoms. Cluster of differentiation 26 (CD26) is also recommended as a potential receptor for SARS-COV-2 [22, 26]. Intriguingly, both ACE2 and CD26 show associations with senescence and immunoregulation.
ACE2, which is widely distributed in the heart, kidneys, lungs, liver, intestine, brain and testes, is a known crucial component of the renin-angiotensin system (RAS)[27]. According to Khemais-Benkhiat et al., RAS is upregulated in endothelial cells with premature and replicative senescence [28]. It has been suggested that differential levels of ACE2 in human organs, especially the cardiac and pulmonary tissues of younger versus older adults, may be responsible for the disease virulence spectrum observed in COVID-19 patients [29]. Ziegler et al. discovered that ACE2 was a human interferon-stimulated gene in airway epithelial cells. SARS-CoV-2 could enhance infection through species-specific interferon-driven upregulation of ACE2 [30]. Smith et al. also identified ACE2 as an interferon-stimulated gene in lung cells. They found that chronic smoke exposure and inflammatory signaling could increase ACE2 expression levels in the respiratory tract. Their findings suggested that SARS-CoV-2 infections could create positive feedback loops that increase ACE2 expression and promote viral dissemination [31].
Interestingly, it has been previously established that ACE2 shows a protective effect in the lungs and that ACE2 expression in the lungs decreases during aging. The lower ACE2 level in the lungs may contribute to the poor prognosis of SARS in the aged group [32]. According to previous research, following SARS-COV entry, ACE2 expression is downregulated dramatically, which leads to a compensatory overproduction of angiotensin 2 (AngII), therefore increasing lung vascular permeability and aggravating lung failure [33]. A similar phenomenon is also observed in SARS-CoV-2-infected lung tissue [34]. According to Datta et al., SARS-CoV-2infects ACE2-expressing cells in the lung, inducing shedding of ACE2 from the cells and, thus, effectively reducing ACE2 expression levels [35]. These findings support the proposed role of ACE2 downregulation in both the pathogenesis and progression into ARDS in SARS and COVID-19 patients.
The contradictions between these research results indicate that SARS-CoV-2 regulation of ACE2 may be complex and dynamic. Whether the regulatory mechanism of SARS-CoV-2 toward ACE2 differs due to the patients’ age, underlying diseases, and stages of infection requires further exploration.
ACE2 is enriched in the heart and plays an essential role in the regulation of heart function [36]. Burrell et al. indicated that ACE2 expression is increased in myocardial infarction in humans and rats [37]. Chen et al. performed state-of-the-art single-cell atlas analysis of the adult human heart and revealed pericytes with high expression levels of ACE2 as target cells of SARS-CoV-2. Patients with coronary heart disease (CHD) showed increased ACE2expression at the mRNA and protein levels [38]. Patients with CHD and infected with SARS-CoV-2 are at an elevated risk of progressing into severe disease [11, 29]. Conversely, acute cardiac injury is reported as one of the most common complications in COVID-19 patients, which significantly exacerbates disease severity [39]. This evidence suggests that enrichment of ACE2 in the myocardium makes the heart one of the main target organs for SARS-CoV-2 infection. The expression level of ACE2 in cardiomyocytes is closely related to the poor prognosis of COVID-19 patients with heart diseases and the severity of COVID-19-induced heart injury.
Cytokine storms, namely, hypercytokinemia, a frequent feature of severe SARS, MERS, H5N1 influenza and H7N9 influenza, are associated with disease severity and are a predictor of prognosis [40-42]. Accumulating data suggest that depletion of lymphocytes, activation of cytotoxic T-lymphocytes, neutrophils and neutrophil-mediated cytokine storms may play key roles in COVID-19 pathogenesis [43]. COVID-19 results in increased levels of plasma cytokines, including interleukin-6 (IL-6), interleukin-1β (IL-1β), interleukin-7 (IL-7), interleukin-8 (IL-8), interleukin-9 (IL-9), interleukin-10 (IL-10), granulocyte colony stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), interferon-γ (IFN-γ), tumor necrosis factor (TNF-α) and vascular endothelial growth factor A (VEGFA). ICU patients with COVID-19 produced higher levels of IL-6 than those not requiring ICU care [44]. According to a meta-analysis, mean IL-6 serum levels are2.9 times higher in patients with severe disease than in those with nonsevere disease [45]. HighIL-6 levels are closely correlated with the serum SARS-CoV-2 viral load, which further affects vital signs and the occurrence of ARDS inCOVID-19 patients [46]. Moreover, as a mediator of SASP, IL-6 is the main functional marker of cell aging [5, 47], and the increase in IL-6 content may correspond to the age-dependent increase in mortality of COVID-19 patients [48].
ACE2 participates in the RAS and plays an important role in regulating IL-6-induced inflammatory injury through the NF-κB and STAT3 pathways [49]. Kubaet al. indicated that SARS-CoV infection could cause a reduction of ACE2 levels on cells, followed by increased serum AngII levels [50]. AngII is one of the key activators of NF-κB and STAT3, which stimulates the expression of IL-6[51]. In turn, we speculate that severe lung inflammation induced by SARS-CoV-2 infection may induce the dysregulation of the RAS followed by the development of ARDS.
CD26, also known as dipeptidyl peptidase 4 (DPP4), is a serine exopeptidase that is expressed ubiquitously in human tissues, including lung, kidney, liver, gut, and immune cell s(including T-cells, activated B-cells, activated natural killer cells and myeloid cells) [52, 53]. CD26 plays multiple roles in nutrition, metabolism, and the immune and endocrine systems. Using mass spectrometry analysis, Kim et al. identified CD26 as a surface protein that is expressed at significantly higher levels in senescent cells. CD26 activity is higher in older than in younger individuals [54]. Overly upregulated CD26 expression and activity are associated with diabetes, obesity and metabolic syndrome, which are reported to influence COVID-19 severity [22, 55].
Moreover, CD26 has been identified as the functional receptor of MERS-CoV [56, 57]. Research has indicated that MERS-CoV is associated with higher mortality among elderly populations with chronic debilitating diseases including diabetes, malignancy, pulmonary and renal diseases. MERS also appears with greater severity and higher mortality rates in elderly people, especially those with debilitated immune systemsorpre-existing comorbidities [58-60]. Therefore, we suggest that similar to the case for ACE2, DPP4 upregulation may be adeterminant of COVID-19 progression and prognosis.
Large numbers of studies have demonstrated the integral role of CD26 in T lymphocyte activation during immunesenescence and costimulation [61]. CD26 acts as a costimulatory agent that mediates T cell activation by binding to the ligand adenosine deaminase [62]. Additionally, CD26 enhances lymphocyte proliferation independent of ADA [63].
CD26 can exist in a soluble form that is considered to be released from the membrane into the plasma, which still retains its enzymatic activity[64]. Ikeda et al. found that soluble CD26 enhances the binding of transcription factors to the TNF-α and IL-6 promoters, thus increasing TNF-α and IL-6 mRNA and protein expression in THP-1 cells [65]. CD26 inhibitors decrease the concentration of proinflammatory factors, such as TNF-α and IL-6 [66]. Thus, some researchers have suggested that the activation of CD26 on T lymphocytes may partially contribute to the high expression of IL-6 in COVID-19 patients. However, the specific role of CD26 in COVID-19 still requires further exploration (Figure 1).
Figure1. Interaction of SARS-CoV-2 with ACE2 and CD26. To enter the host cells, SARS-CoV-2 binds to membrane-bound ACE2 with the assistance of Furin and TMPRSS2. SARS-CoV-2 infections could create positive feedback loops that increase ACE2 expression and promote viral dissemination. On the other hand, SARS-CoV-2 infections may induce ACE2 shedding. ACE2 downregulation could lead to accumulation of Ang II, therefore inducing cytokine storm and ARDS. Activation of CD26 on T lymphocytes may partially contribute to the high expression of IL-6 in COVID-19 patients.
Proposed clinical applications in elderly covid-19 patients
Current evidence suggests that elderly patients with past comorbidities or dyspnea should be closely monitored for signs of disease progression, decompensation, and exacerbation of illness, especially 1-2 weeks after the onset of symptoms[10, 67]. Presently, there are no officially approved medicines available against SARS-CoV-2. Although the management of COVID-19 patients is primarily supportive, specific therapies are still under investigation. These therapies include current and potential antiviral drugs, anti-senescence drugs, immunosuppressive agents, steroids, mesenchymal stem cell (MSC) transplantation, and an artificial liver system (ALS), among others (Table 1). In the following paragraphs, we aim to highlight the proposed therapeutic strategies [68].
Antiviral drugs
Timely antiviral therapy is highly recommended early the course of COVID-19 patients, especially elderly patients and patients with underlying conditions. Wu et al. retrospectively investigated the clinical data of 280 COVID-19 cases and recommended that timely antiviral treatment should be initiated to slow disease progression and improve prognosis in elderly patients [2]. Previously, oseltamivir, which could reduce the mortality of influenza patients, and ganciclovir, which is primarily used to treat cytomegalovirus [69], were widely used for SARS-CoV-2 patients. However, the efficiencies of neuraminidase inhibitors are currently being questioned, which makes them beyond recommendation [70, 71].
Remdesivir (GS-5734) is a monophosphoramidate prodrug of an adenosine analog that can affect viral RNA polymerase and reduce the production of viral RNA [72]. Remdesivir has shown a significant therapeutic effect in MERS-CoV mouse models [73]. It is effective in the EC50 range of 0.069 μM for SARS-CoV and 0.074 μM for MERS-CoV in tissue cultures as well as 0.77 μM in Vero E6 cells [72, 74]. Theoretically, remdesivir is currently the most promising drug for treating COVID-19. According to the result of a prospective, open-label study of remdesivir, Antinori et al. indicated that this drug could benefit hospitalized patients with SARS-CoV-2 pneumonia, with fewer adverse events observed [75]. The clinical trial conducted by Wang et al. in 237 patients at ten hospitals in Hubei Province showed that, although not statistically significant, the patients receiving remdesivir had a faster time to clinical improvement than those receiving placebo [76]. In the trial conducted by Beigel and colleagues, 1063 COVID-19 patients were randomly assigned to remdesivir or placebo. The results showed that remdesivir could obviously shorten the recovery time in hospitalized COVID-19 patients [77]. The authors also emphasized that earlier remdesivir treatment was probably more beneficial than later treatment [78]. Further explorations of the safety and efficiency of remdesivir for COVID-19 are still ongoing.
Table 1
Table 1 Potential strategies for the treatment of COVID-19.
Treatment
Agent
Related Target/Pathways
Potential efficacy in COVID-19
Antiviral drugs
Remdesivir LPV/RTV Favipiravir Arbidol
Reduces the production of viral RNA Inhibits antiretroviral protease Targets RNA-dependent RNA polymerase Perturbs the virus membrane structure
Shortens the recovery time in COVID-19 patients Shortens the viral shedding duration in patients Induces a shorter viral clearance time and greater improvement rate in chest imaging Shorter duration of positive RNA test compared to those treated with LPV/RTV
Targets and removes senescent cells; inhibits IL-6 and IL-1β expression; extends the lifespan of myofibroblasts Prevents the induction and accumulation of β-Gal; inhibits the replication of SARS-CoV in vitro Downregulates the IL-6 pathway; reduces the number of senescent T-cells through the mTOR-NLRP3-IL-1β axis
Reduces airway inflammation; antifibrosis Reduces the viral load in COVID-19 patients Prevents and treats the severity of COVID-19 patients
ACE2-related therapy
ACE2 activator ACE2 inhibitor Human recombinant soluble ACE2
Avoids binding of S protein of SARS-CoV-2 to ACE2 Inhibits ACE2 expression Directly binds to SARS-CoV-2 in the circulation
Requires scientific and clinical evidence Still under debate Blocks SARS-CoV-2 infection; prevents lung injury
CD26 inhibitor
Linagliptin
Attenuates DM-induced activation of NLRP3 inflammatory bodies
Decreases the concentration of cytokines, especially TNF-α and IL-6
Immunosuppressive Therapy
Tocilizumab; sarilumab; siltuximab cyclosporine-cyclophilin A complex Corticosteroids
Directly targets IL-6 receptors Halts the expression of TNF-α and IL-2; blocks the replication of coronaviruses Inhibits innate and adaptive immune responses as well as immune cells
Improves clinical outcomes in severe cases Anti-inflammatory and antiviral properties in COVID-19 Improves clinical outcomes in COVID-19 patients with ARDS
MSC transplantation
/
Advantages in anti-inflammation, antifibrosis and injury repair
Improves pulmonary function and symptoms of patients
Artificial liver system
/
Attenuates the cytokine storm
Reduces the mortality of severe patients exhibiting rapid disease progression
Lopinavir/ritonavir (LPV/RTV),which acts as antiretroviral protease inhibitor, is used as an anti-HIV drug [79]. In India, the Central Drugs Standard Control Organization approved the restricted public health use of the LPV/RTV combination in symptomatic COVID-19 patients [80]. However, the efficacy of LPV/RTV for COVID-19 is still controversial. A clinical trial in Hubei showed that early LPV/RTV treatment could shorten the viral shedding duration in COVID-19 patients, especially in those of an older age [81]. Cheng et al. obtained the exact opposite result among patients with mild pneumonia in Taiwan [82]. According to a randomized, controlled, open-label trial in 199 patients with severe COVID-19, mortality at 28 days and viral clearance time were similar in the LPV/RTV group and the standard-care group. The results suggested that no benefit was observed with LPV/RTV treatment [74]. Therefore, the WHO suggested larger trials with a greater variety of COVID-19 patients [83].
Favipiravir (FPV), a purine nucleic acid analog that targets RNA-dependent RNA polymerase (RdRP), is widely used as an oral anti-influenza drug [84]. Cai et al. conducted a clinical trial to evaluate the safety and efficacy of favipiravir in COVID-19 patients. A shorter viral clearance time as well as a significantly higher improvement rate in chest imaging was shown for the FPV group versus the LPV/r group. In addition, fewer adverse reactions were found in the FPV group than in the LPV/r group [85].
Arbidol, an important anti-viral drug candidate, also showed promising effects in COVID-19. Arbidol is a broad-spectrum antiviral molecule that inhibits both DNA as well as RNA viruses by altering the membrane structure of the virus [86]. According to Zhu et al., patients treated with arbidol show a shorter duration of positive RNA test compared to those treated with LPV/RTV, while nosignificant adverse effects are observed. The results indicated that arbidol monotherapy is superior to LPV/RTVin COVID-19 treatment [87]. Additionally, a retrospective cohort study showed that arbidol combined with LPV/RTV showed improved efficacy in COVID-19 patients [88]. Another retrospective, single-center study showed that the combination of Lianhuaqingwen and arbidol was effective for patients with mild symptoms within 5-7 days, and the cure rate was 98% [89]. Moreover, arbidol is considered to have a preventive effect. Yang et al. suggested that prophylactic oral arbidol was associated with a lower incidence of SARS-CoV-2 infection in medical staff [90]. Although accumulating evidence has demonstrated the potential clinical efficiency of arbidol, powered randomized control trials are still needed for further confirmation [91].
Antisenescence drugs
Azithromycin and the closely related drug roxithromycin are macrolide antibiotics that can act as senolytic drugs that target and remove senescent cells [92]. Additionally, azithromycin is known to exert an antifibrotic effect by significantly extending the lifespan of myofibroblast cells. Moreover, azithromycin has been proven to reduce airway inflammation by inhibiting IL-6 and IL-1β expression in mouse models [93, 94]. Therefore, azithromycin is recommended by a number of researchers as a potential COVID-19 treatment strategy. However, Gbinigie et al. conducted a rapid review of the current literature. The results indicated that other than in the case of bacterial super infection, there was no evidence supporting the use of azithromycin for the treatment of SARS-CoV-2 infection outside of the context of clinical trials [95]. According to a clinical trial conducted by Rosenberg et al., receipt of azithromycin alone could not significantly reduce in-hospital mortality of COVID-19 patients [96].
Chloroquine (CQ) and its derivative hydroxychloroquine (HCQ) have the ability to induce alkalization, which functionally prevents the induction and accumulation of beta-galactosidase (β-Gal), known as a marker of senescence [97]. CQ and HCQ are widely used antimalarial and antiviral drugs and have recently received much attention as potential treatments for COVID-19 [98].CQ was recently demonstrated as an inhibitor ofSARS-CoV-2 in vitro, and the hydroxylated form, HCQ, has been proven to limit the replication of SARS-CoV-2 in vitro [99, 100]. Huang et al. found that CQ had a slight advantage over lopinavir/ritonavir in COVID-19 patients [101]. HCQ can also specifically inhibit the replication of SARS-CoV by interfering with the glycosylation of ACE2 [102]. Therefore, HCQ has been widely suggested as a potential treatment for patients with SARS-CoV-2 infection. A number of clinical trials have been conducted to explore the efficacies of CQ and HCQ. According to a small open-label nonrandomized clinical trial, HCQ treatment was significantly associated with viral load reduction in COVID-19 patients, and its efficacy could be reinforced by azithromycin [103]. However, according to a newly published comparative observational study among 181 COVID-19 patients with documented severe acute respiratory syndrome who required oxygen, HCQ did not show an obvious therapeutic effect. Additionally, eight patients in the HCQ group (10%) experienced electrocardiographic modifications that required discontinuation of treatment [104]. Despite the controversial results of these clinical trials, frequent side effects of CQ and HCQ, for example, worsening vision, nausea, digestive disorders and potential heart failure and even death, have hindered the wide application of these drugs [105]. Moreover, the results of a clinical trial conducted by Rosenberg et al., which involved 1438 COVID-19 patients, showed that compared with neither treatment, treatment with HCQ alone or combined with azithromycin was not significantly associated with differences in mortality [96].
Rapamycin is widely known as a key anti-aging drug and prevents the progression of senescence in human cell lines and animal models [106-108]. Rapamycin acts as an inhibitor of protein synthesis, inhibiting cytokine expression and viral replication [109]. In elderly patients, especially those with CHD or reduced T-cell counts, rapamycin can significantly reduce the expression of the serum senescence marker IL-6 [110]. As a candidate for potential use in COVID-19, rapamycin may prevent progression to severe forms of COVID-19 by downregulating the IL-6 pathway and reducing the number of senescent T-cells through the mTOR-NLRP3-IL-1β axis at the early stage of cytokine storms [111, 112]. Conversely, rapamycin is suggested as a novel intervention strategy beyond vaccines to prevent severe symptoms in COVID-19 [113]. Therefore, conducting clinical trials for rapamycin to prevent and treat the severity of COVID-19 patients, especially elderly patients, is strongly recommended.
ACE2-related therapies
Some researchers have suggested that SARS-CoV-2 induces initial damage effects by downregulating ACE2 expression and blocking ACE2-mediated activity and activating ACE2 may be much more efficacious. Accumulating evidence has illustrated that the activation of ACE2 could be a positive treatment method. ACE2 activators are purported to have two therapeutic effects: avoiding the binding of the S protein of SARS-CoV-2 to ACE2 and promoting the protective effects of different organs, preventing lung injury and fibrosis [34, 114, 115].ACE2 activators, such as diminazene aceturate, are recommended for application in COVID-19 patients [34].
However, due to the positive-feedback loop between virus infection and ACE2 expression, some researchers have suggested the use of ACE2 inhibitors to block SARS-CoV-2 infection. Considering the role of ACE2 in maintaining organ functioning, especially in the lungs, the clinical application of ACE2 inhibitors in COVID-19 is under question [116]. The findings regardingACE2 have sparked a debate regarding the potential use of angiotensin-converting enzyme inhibitors (ACEIs) and AngII receptor blockers (ARBs) among elderly COVID-19 patients in the context of the pandemic [117]. However, after reviewing published relevant animal, in vitro and clinical studies, Chung et al. announced that the results did not show a higher risk of infection with ACEI or ARB use [118]. Considering the contradictory hypotheses and lack of scientific evidence and clinical data worldwide, the European Society of Cardiology and the American College of Cardiology recommended the continuation of ACEIs or ARBs for COVID-19 patients who were already taking these medicines [119, 120].
Human recombinant soluble ACE2 (hrsACE2) is an FDA-approved treatment, with a 2017 phase II trial for ARDS [121]. Circulating soluble ACE2 can bind to SARS-CoV-2 but is unable to inhibit cell infection [122]. According to Monteil et al., clinical grade hrsACE2 reduces SARS-CoV-2 recovery from Vero cells by 1,000-5,000 times, demonstrating that hrsACE2 can not only block SARS-CoV-2 infection but also protect against lung injury, suggesting a possible therapeutic approach [123].
CD26 inhibitors
The clinical immune response to SARS-CoV-2 can be divided into 2 phases: an earlier phase of elimination by antiviral adaptive immunity and a later phase of damaged alveolar cells triggering innate inflammation [124]. According to Chen et al., the occurrence of ARDS may be associated with the later immune phase, and treatment to reduce inflammation during that phase may help reduce lung damage. CD26 inhibitors may potentially act to regulate an overactive immune reaction and prevent devastating lung injury [125]. In a mouse model of ARDS, which is the main cause of death in COVID-19 patients, CD26 inhibition by sitagliptin alleviated histological findings of lung injury by inhibiting the expression of IL-1β, TNF-α, and IL-6[126]. Birnbaum et al. reported that saxagliptin-mediated DPP4 inhibition could attenuate diabetes mellitus (DM) -induced activation of nod-like receptor family pyrin domain-containing 3 (NLRP3) inflammatory bodies, thus reducing serum CRP, TNF-α, IL-1β, IL-18 and IL-6 levels [127]. CD26 inhibitors, including sitagliptin, alogliptin, vildagliptin, saxagliptin, and linagliptin, are a class of drugs used effectively in the treatment of type 2 diabetes, which has demonstrated safety in elderly patients. These drugs have similar effects by binding to essentially the same catalytic site [128]. Research has shown that the administration of linagliptin can lead to a decrease in the concentration of proinflammatory factors, especially TNF-α and IL-6 [66]. Moreover, mathematical modeling has shown that the spread of MERS-CoV infection can be controlled by inhibiting the expression of CD26, with similar efficiency in SARS-CoV-2 infection [129]. Since the expression of CD26 is closely related to the pathogenesis and severity of COVID-19, CD26 inhibitors have recently been proposed as potential drugsagainst COVID-19 [130]. However, despite laboratory verification and theoretical feasibility, the actual efficacies of CD26 inhibitors in COVID-19 still require verification in further clinical trials.
Immunosuppressive agents
As we mentioned above, COVID-19 severity and outcomes are closely related to the characteristics of the immuneresponse and subsequent cytokine storm incited by pathogenic T cells and inflammatory monocytes with a high level of IL-6 secretion, which are more severe in elderly patients [131]. Some researchers have recommended monoclonal antibodies that target IL-6,TNF-α and other cytokine pathways as a potential strategy to attenuate the inflammatory storm [132].
Tocilizumab is a marketed humanized monoclonal antibody that directly targets IL-6 receptors. Accumulating clinical trials have confirmed its safety and effectiveness in rheumatoid arthritis treatment. In a clinical trial among 45 patients, tocilizumab exerted a rapidly beneficial effect on fever and inflammatory markers in COVID-19 patients [133]. According to Xu et al., within 5 days after additional application of tocilizumab, the percentage of lymphocytes in peripheral blood returned to normal in 52.6% of severe COVID-19 patients, and all patients were discharged after anaverage of 15.1 days. The results indicated that tocilizumab could improve the clinical outcomes in severe COVID-19 patients by suppressing the immune response [131]. Recently, tocilizumab was approved for patients with severe SARS-CoV-2 pulmonary complications by the National Health Commission of the People’s Republic of China. Other monoclonal antibodies specifically targeting IL-6 pathways, such as sarilumab and siltuximab, are also recommended for COVID-19 treatment. Clinical trials are still needed to evaluate their efficacy and safety in COVID-19 patients.
The cyclosporine-cyclophilin A complex, including cyclophilin and tacrolimus, is considered to suppress organ rejection by halting the expression of TNF-α and IL-2 [134]. Moreover, according to Pfefferle et al., cyclophilin can block the replication of coronaviruses, including SARS-CoV, human CoV-229E and CoV-NL-63, feline CoV, among others. These results suggest that cyclophilin is a broad-spectrum coronavirus inhibitor and might be used for therapy in emerging coronavirus infections [135]. Therefore, the anti-inflammatory and antiviral properties of the cyclosporine-cyclophilin A complex make it a potential clinical application in severe COVID-19. However, considering the nephrotoxicity and hepatotoxicity of cyclophilin and tacrolimus, safety issues must be explored in COVID-19 patients, especially elderly individuals with liver and kidney involvement.
Corticosteroids show inhibitory effects on both innate and adaptive immune responses, as well as multiple types of immune cells [136]. Corticosteroids were among the first therapies tested in trials for preventing ARDS [137]. Meduri et al. constructed a clinical trial to investigate the efficacy of long-term corticosteroid treatment in patients with ARDS. The results showed that prolonged corticosteroid application could accelerate the resolution of ARDS and decrease hospital mortality [138]. Fadel et al. conducted a single pretest, single posttest quasi-experiment among 213 COVID-19 patients. The results indicated that an early short course of methylprednisolone application could reduce escalation of care and improve clinical outcomes in patients with moderate-to-severe COVID-19 [139]. However, clinical management of severe SARS and MERS patients revealed that corticosteroid therapy did not decrease mortality; in contrast, it caused delayed viral shedding [140]. In addition, Zha et al. announced that after analyzing the data of 31 COVID-19 patients, they found no association between corticosteroid therapy and outcomes in patients without ARDS [141]. The efficacy of corticosteroids in COVID-19 patients remains controversial. Thus, the Guideline for the Diagnosis and Treatment of COVID-19 (7th version) recommended low-to-moderate doses and short courses of corticosteroid application in selected COVID-19 cases that represent excessive immune response activation or rapid progression of imaging changes
MSC transplantation
MSCs are nonhematopoietic stem cells derived from the mesoderm, which can be isolated from various tissues, such as bone marrow, adipose tissue, umbilical cord blood, placenta, menstrual blood, dental pulp, and amniotic fluid [142]. Accumulating evidence from preclinical and clinical trials has demonstrated that MSCs have great advantages in anti-inflammation, anti-fibrosis and injury repair [143-145]. Shao et al. reported that MSCs could strongly suppress IL-6 production, thereby disrupting the development of cytokine storms [146]. Previously, it was demonstrated that MSC transplantation could significantly reduce the mortality of patients with H7N9-induced ARDS (17.6% died in the MSC group, whereas54.5% died in the control group). Moreover, no significant adverse effects were observed in these patients [147]. According to Leng et al., MSC transplantation could significantly improve pulmonary function and symptoms of COVID-19 patients without obvious adverse effects. Moreover, decreased TNF-α and increased IL-10 levels were detected in the MSC treatment group compared with the control group [148]. These results indicated that MSC-based therapy could be a potential alternative for managing patients with severe symptoms of COVID-19.
Artificial liver system
The artificial liver system (ALS) is widely used as an effective support therapy in severe liver failure patients [149]. As mentioned above, the cytokine storm is the main motivator of COVID-19 progression and a poor prognosis, and its severity is closely associated with advanced age. Previously, clinical trials have demonstrated that the plasma exchange module of ALS exhibited high efficacy in attenuating the cytokine storm of H7N9 infection [150]. A single-center study showed that artificial liver plasma exchange could significantly reduce inflammatory cytokine levels, thus reducing mortality in critically ill patients with COVID-19 [151]. Our colleagues found that the application of ALS showed excellent prognosis in the treatment of severeCOVID-19 patients presenting a cytokine storm [152]. According to the Diagnosis and Treatment of COVID-19 (7th version) published in China, ALS is recommended in patients who exhibit rapid disease progression confirmed by lung imaging and a cytokine storm.
Nutritional support in elderly people
To date, considerable evidence has demonstrated that food and nutrients could affect immune system function. Poor nutritional status is widely considered one of the significant risk factors for severe COVID-19 [153]. It has been directly highlighted that nutritional support may play an important role in determining COVID-19 outcomes [154]. Generally, there are nutritional deficiencies in calcium, vitamin C, vitamin D, folate, and zinc among the elderly population, especially among in-hospital patients [155]. According to a study in Wuhan, the prevalence of malnutrition is elevated in elderly patients with COVID-19 [156]. The researchers suggested that nutritional support should be strengthened during treatment. Malnutrition can exacerbate the immune system deficiency in elderly individuals, making them susceptible to SARS-CoV-2 infection [157]. A healthy, balanced diet can provide elderly individuals with necessary macro- and micronutrients, prebiotics, probiotics, and symbiotics to restore and maintain immune cell function, thus reducing the incidence of SARS-CoV-2 infection [153].
Problems faced by the progress and application of the vaccine
The development of a safe and effective vaccine against SARS-CoV-2 for nonimmune individuals is an urgent and critical task for controlling the ongoing pandemic [68]. The developing coronavirus vaccines and drugs mainly target the spike glycoprotein or S protein, the major inducers of neutralizing antibodies. To date, Wei Chen et al. conducted a dose-escalation, single-center, open-label, nonrandomized, first-in-human trial of a recombinant adenovirus type5-vectored COVID-19 vaccine in Wuhan, China. The vaccine was tolerable and immunogenic 28 days after vaccination. The humoral responses against SARS-CoV-2 peaked at day 28 after vaccination in healthy adults, and rapid specific T-cell responses were noted from day 14 after vaccination [158].
However, even if a successful vaccine for SARS-CoV-2 becomes available, an individual’s immune response must be sufficiently strong to respond to the vaccine, and once exposure occurs, the reaction can later confer protection against the pathogen. Thus, vaccines cannot provide complete protection in elderly populations due to age-related declines in immune function and the accumulation of various diseases. According to Montoet al., influenza outbreaks still occur in elderly nursing homes even when vaccination rates reach 80-98% utilization [159]. Thus, the deficiency of the elderly group could become a gap in herd immunity that relies on vaccines. Some researchers recommended remodeling of the senescent immune system of elderly persons by allo-priming as a method to restore cellular immune function. Heterologous immunity can enhance the panviral protection upon each viral exposure, thereby providing long-term protection. The alloantigen priming strategy has been proposed in conjunction with viral-specific vaccines in the elderly population [160]. However, the efficiency requires further exploration.
Moreover, accumulating reports worldwide of some COVID-19 patients testing positive again after initially testing negative indicate the potential of re-infections and short-lasting immunity against COVID-19 [161]. To et al. firstly reported the case of COVID-19 re-infection by a phylogenetically distinct SARS-corona-virus-2 strain [162]. According to Ibarrondo et al., antibody loss in COVID-19 patients is quicker than that reported for SARS-CoV [163]. It means that humoral immunity against SARS-CoV-2 may not be long lasting in human bodies. Consequently, people doubt whether the vaccine could produce long-term immunity in the population.
Conclusions
The COVID-19 pandemic suggests that we are facing a historic challenge to our capacity to protect the health of our elderly population. Protecting aging populations is now a central question in maintaining global health and biosecurity [4]. Lloyd-Sherlock et al. announced that due to great barriers in access to health services and support, older people in low-and middle-income countries are bearing the brunt of COVID-19 [164]. An open letter suggested that the WHO should act immediately to redress its neglect of older people, and member states must prioritize the needs of the elderly population in national responses and support for low- and middle-income countries [165]. The current results of biomedical, clinical and public health studies also highlight the need for therapy and prevention strategies for aging COVID-19 patients. We hope that this review can provide insight regarding the prevention and treatment of COVID-19 in elderly populations.
Acknowledgement
This study was supported by the National Key Research and Development Program of China (2016YFC 1101304/3) and Zhejiang Province Key Research and Development Plan Emergency Project (No. 2020C03123-1).
ToKK, TsangOT, LeungWS, TamAR, WuTC, LungDC, et al. (2020).
Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: an observational cohort study
ZhengS, FanJ, YuF, FengB, LouB, ZouQ, et al. (2020).
Viral load dynamics and disease severity in patients infected with SARS-CoV-2 in Zhejiang province, China, January-March 2020: retrospective cohort study
ZhouL, NiuZ, JiangX, ZhangZ, ZhengY, WangZ, et al. (2020).
Systemic analysis of tissue cells potentially vulnerable to SARS-CoV-2 infection by the protein-proofed single-cell RNA profiling of ACE2, TMPRSS2 and Furin proteases
Khemais-BenkhiatS, Idris-KhodjaN, RibeiroTP, SilvaGC, AbbasM, KheloufiM, et al. (2016).
The Redox-sensitive Induction of the Local Angiotensin System Promotes Both Premature and Replicative Endothelial Senescence: Preventive Effect of a Standardized Crataegus Extract
Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases From the Chinese Center for Disease Control and Prevention
Binding to human dipeptidyl peptidase IV by adenosine deaminase and antibodies that inhibit ligand binding involves overlapping, discontinuous sites on a predicted beta propeller domain
YuDM, SlaitiniL, GysbersV, RiekhoffAG, KahneT, KnottHM, et al. (2011).
Soluble CD26 / dipeptidyl peptidase IV enhances human lymphocyte proliferation in vitro independent of dipeptidyl peptidase enzyme activity and adenosine deaminase binding
WicinskiM, GorskiK, WalczakM, WodkiewiczE, SlupskiM, Pawlak-OsinskaK, et al. (2019).
Neuroprotective Properties of Linagliptin: Focus on Biochemical Mechanisms in Cerebral Ischemia, Vascular Dysfunction and Certain Neurodegenerative Diseases
AntinoriS, CossuMV, RidolfoAL, RechR, BonazzettiC, PaganiG, et al. (2020).
Compassionate remdesivir treatment of severe Covid-19 pneumonia in intensive care unit (ICU) and Non-ICU patients: Clinical outcome and differences in post-treatment hospitalisation status
BhatnagarT, MurhekarMV, SonejaM, GuptaN, GiriS, WigN, et al. (2020).
Lopinavir/ritonavir combination therapy amongst symptomatic coronavirus disease 2019 patients in India: Protocol for restricted public health emergency use
YanD, LiuXY, ZhuYN, HuangL, DanBT, ZhangGJ, et al. (2020).
Factors associated with prolonged viral shedding and impact of Lopinavir/Ritonavir treatment in hospitalised non-critically ill patients with SARS-CoV-2 infection
SARS-CoV-2: Recent Reports on Antiviral Therapies Based on Lopinavir/Ritonavir, Darunavir/Umifenovir, Hydroxychloroquine, Remdesivir, Favipiravir and Other Drugs for the Treatment of the New Coronavirus
MahevasM, TranVT, RoumierM, ChabrolA, PauleR, GuillaudC, et al. (2020).
Clinical efficacy of hydroxychloroquine in patients with covid-19 pneumonia who require oxygen: observational comparative study using routine care data
BergerJP, SinhaRoyR, PocaiA, KellyTM, ScapinG, GaoYD, et al. (2018).
A comparative study of the binding properties, dipeptidyl peptidase-4 (DPP-4) inhibitory activity and glucose-lowering efficacy of the DPP-4 inhibitors alogliptin, linagliptin, saxagliptin, sitagliptin and vildagliptin in mice
ChenJ, HuC, ChenL, TangL, ZhuY, XuX, et al. (2020).
Clinical study of mesenchymal stem cell treating acute respiratory distress syndrome induced by epidemic Influenza A (H7N9) infection, a hint for COVID-19 treatment
ZhuFC, LiYH, GuanXH, HouLH, WangWJ, LiJX, et al. (2020).
Safety, tolerability, and immunogenicity of a recombinant adenovirus type-5 vectored COVID-19 vaccine: a dose-escalation, open-label, non-randomised, first-in-human trial
Individual risk management strategy and potential therapeutic options for the COVID-19 pandemic
1
2020
... Coronavirus disease 2019 (COVID-19) is an emerging respiratory infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which was first identified in mid-December 2019 in Wuhan, China. Currently, it has spread globally and been declared a pandemic by the World Health Organization (WHO). Up to August 18,2020, more than 767,000 deaths and 21,500,000 confirmed positive cases have been reported around the world. Accumulating evidence shows that age and underlying conditions of virus contacts are crucial factors influencing personal fate toward different clinical severities of COVID-19, ranging from asymptomatic, mild, and moderate to death [1, 2]. COVID-19 shows a considerably elevated mortality rate in patients with advanced age and pre-existing comorbidities [3]. Under the situation of global aging, the COVID-19 pandemic creates challenges for not only widespread public health but also biomedical and clinical aging research [4]. ...
Early antiviral treatment contributes to alleviate the severity and improve the prognosis of patients with novel coronavirus disease (COVID-19). J
2
2020
... Coronavirus disease 2019 (COVID-19) is an emerging respiratory infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which was first identified in mid-December 2019 in Wuhan, China. Currently, it has spread globally and been declared a pandemic by the World Health Organization (WHO). Up to August 18,2020, more than 767,000 deaths and 21,500,000 confirmed positive cases have been reported around the world. Accumulating evidence shows that age and underlying conditions of virus contacts are crucial factors influencing personal fate toward different clinical severities of COVID-19, ranging from asymptomatic, mild, and moderate to death [1, 2]. COVID-19 shows a considerably elevated mortality rate in patients with advanced age and pre-existing comorbidities [3]. Under the situation of global aging, the COVID-19 pandemic creates challenges for not only widespread public health but also biomedical and clinical aging research [4]. ...
... Timely antiviral therapy is highly recommended early the course of COVID-19 patients, especially elderly patients and patients with underlying conditions. Wu et al. retrospectively investigated the clinical data of 280 COVID-19 cases and recommended that timely antiviral treatment should be initiated to slow disease progression and improve prognosis in elderly patients [2]. Previously, oseltamivir, which could reduce the mortality of influenza patients, and ganciclovir, which is primarily used to treat cytomegalovirus [69], were widely used for SARS-CoV-2 patients. However, the efficiencies of neuraminidase inhibitors are currently being questioned, which makes them beyond recommendation [70, 71]. ...
Clinical characteristics of 113 deceased patients with coronavirus disease 2019: retrospective study
1
2020
... Coronavirus disease 2019 (COVID-19) is an emerging respiratory infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which was first identified in mid-December 2019 in Wuhan, China. Currently, it has spread globally and been declared a pandemic by the World Health Organization (WHO). Up to August 18,2020, more than 767,000 deaths and 21,500,000 confirmed positive cases have been reported around the world. Accumulating evidence shows that age and underlying conditions of virus contacts are crucial factors influencing personal fate toward different clinical severities of COVID-19, ranging from asymptomatic, mild, and moderate to death [1, 2]. COVID-19 shows a considerably elevated mortality rate in patients with advanced age and pre-existing comorbidities [3]. Under the situation of global aging, the COVID-19 pandemic creates challenges for not only widespread public health but also biomedical and clinical aging research [4]. ...
Covid-19 and Immunity in Aging Populations - A New Research Agenda
2
2020
... Coronavirus disease 2019 (COVID-19) is an emerging respiratory infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which was first identified in mid-December 2019 in Wuhan, China. Currently, it has spread globally and been declared a pandemic by the World Health Organization (WHO). Up to August 18,2020, more than 767,000 deaths and 21,500,000 confirmed positive cases have been reported around the world. Accumulating evidence shows that age and underlying conditions of virus contacts are crucial factors influencing personal fate toward different clinical severities of COVID-19, ranging from asymptomatic, mild, and moderate to death [1, 2]. COVID-19 shows a considerably elevated mortality rate in patients with advanced age and pre-existing comorbidities [3]. Under the situation of global aging, the COVID-19 pandemic creates challenges for not only widespread public health but also biomedical and clinical aging research [4]. ...
... The COVID-19 pandemic suggests that we are facing a historic challenge to our capacity to protect the health of our elderly population. Protecting aging populations is now a central question in maintaining global health and biosecurity [4]. Lloyd-Sherlock et al. announced that due to great barriers in access to health services and support, older people in low-and middle-income countries are bearing the brunt of COVID-19 [164]. An open letter suggested that the WHO should act immediately to redress its neglect of older people, and member states must prioritize the needs of the elderly population in national responses and support for low- and middle-income countries [165]. The current results of biomedical, clinical and public health studies also highlight the need for therapy and prevention strategies for aging COVID-19 patients. We hope that this review can provide insight regarding the prevention and treatment of COVID-19 in elderly populations. ...
Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study
2
2020
... New coronavirus-exposed populations are generally susceptible, but elderly people, especially those with underlying conditions normally considered to be aging-associated diseases (diabetes, hypertension, and cardiovascular and cerebrovascular diseases), exhibit increased susceptibility [5]. Moreover, the spread of SARS-CoV-2 as well as severe acute respiratory syndrome coronavirus (SARS-CoV) in 2003 made it clear that these aging patients are more likely to progress to severe disease and die more easily from these infections than younger people [6-8]. After analyzing the data for 1099 COVID-19 patients from 552 hospitals in China, Nanshan Zhong et al. found that patients with severe disease were older than those with nonsevere disease and that coexisting illness was more common among patients in the severe group[9]. In the United States, 80% of deaths have occurred in patients over the age of 65 years, and patients aged 85 years and over have a high proportion of severe outcomes, mirroring the experience in China [10]. According to a meta-analysis, serious aging-related chronic diseases(associated with a pathological role of cellular senescence), including hypertension, diabetes, chronic obstructive pulmonary disease (COPD), cardiovascular disease, and cerebrovascular disease, are independent risk factors associated with COVID-19 patients [11]. ...
... Cytokine storms, namely, hypercytokinemia, a frequent feature of severe SARS, MERS, H5N1 influenza and H7N9 influenza, are associated with disease severity and are a predictor of prognosis [40-42]. Accumulating data suggest that depletion of lymphocytes, activation of cytotoxic T-lymphocytes, neutrophils and neutrophil-mediated cytokine storms may play key roles in COVID-19 pathogenesis [43]. COVID-19 results in increased levels of plasma cytokines, including interleukin-6 (IL-6), interleukin-1β (IL-1β), interleukin-7 (IL-7), interleukin-8 (IL-8), interleukin-9 (IL-9), interleukin-10 (IL-10), granulocyte colony stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), interferon-γ (IFN-γ), tumor necrosis factor (TNF-α) and vascular endothelial growth factor A (VEGFA). ICU patients with COVID-19 produced higher levels of IL-6 than those not requiring ICU care [44]. According to a meta-analysis, mean IL-6 serum levels are2.9 times higher in patients with severe disease than in those with nonsevere disease [45]. HighIL-6 levels are closely correlated with the serum SARS-CoV-2 viral load, which further affects vital signs and the occurrence of ARDS inCOVID-19 patients [46]. Moreover, as a mediator of SASP, IL-6 is the main functional marker of cell aging [5, 47], and the increase in IL-6 content may correspond to the age-dependent increase in mortality of COVID-19 patients [48]. ...
SARS: epidemiology
1
2003
... New coronavirus-exposed populations are generally susceptible, but elderly people, especially those with underlying conditions normally considered to be aging-associated diseases (diabetes, hypertension, and cardiovascular and cerebrovascular diseases), exhibit increased susceptibility [5]. Moreover, the spread of SARS-CoV-2 as well as severe acute respiratory syndrome coronavirus (SARS-CoV) in 2003 made it clear that these aging patients are more likely to progress to severe disease and die more easily from these infections than younger people [6-8]. After analyzing the data for 1099 COVID-19 patients from 552 hospitals in China, Nanshan Zhong et al. found that patients with severe disease were older than those with nonsevere disease and that coexisting illness was more common among patients in the severe group[9]. In the United States, 80% of deaths have occurred in patients over the age of 65 years, and patients aged 85 years and over have a high proportion of severe outcomes, mirroring the experience in China [10]. According to a meta-analysis, serious aging-related chronic diseases(associated with a pathological role of cellular senescence), including hypertension, diabetes, chronic obstructive pulmonary disease (COPD), cardiovascular disease, and cerebrovascular disease, are independent risk factors associated with COVID-19 patients [11]. ...
Communicating the Risk of Death from Novel Coronavirus Disease (COVID-19)
0
2020
Exploring the Relevance of Senotherapeutics for the Current SARS-CoV-2 Emergency and Similar Future Global Health Threats
2
2020
... New coronavirus-exposed populations are generally susceptible, but elderly people, especially those with underlying conditions normally considered to be aging-associated diseases (diabetes, hypertension, and cardiovascular and cerebrovascular diseases), exhibit increased susceptibility [5]. Moreover, the spread of SARS-CoV-2 as well as severe acute respiratory syndrome coronavirus (SARS-CoV) in 2003 made it clear that these aging patients are more likely to progress to severe disease and die more easily from these infections than younger people [6-8]. After analyzing the data for 1099 COVID-19 patients from 552 hospitals in China, Nanshan Zhong et al. found that patients with severe disease were older than those with nonsevere disease and that coexisting illness was more common among patients in the severe group[9]. In the United States, 80% of deaths have occurred in patients over the age of 65 years, and patients aged 85 years and over have a high proportion of severe outcomes, mirroring the experience in China [10]. According to a meta-analysis, serious aging-related chronic diseases(associated with a pathological role of cellular senescence), including hypertension, diabetes, chronic obstructive pulmonary disease (COPD), cardiovascular disease, and cerebrovascular disease, are independent risk factors associated with COVID-19 patients [11]. ...
... Senescent cells accumulate with age in vertebrates and promote aging mainly through the senescence-associated secretory phenotype (SASP) [20]. Data have shown that RNA viruses, such as influenza virus, display enhanced replication efficiency in senescent cells, which suggests that the accumulation of senescent cells in aging and age-related diseases may play a role in this phenomenon. However, the response to SARS-COV-2 that occurs in senescent cells is still poorly understood [8]. ...
Clinical Characteristics of Coronavirus Disease 2019 in China
1
2020
... New coronavirus-exposed populations are generally susceptible, but elderly people, especially those with underlying conditions normally considered to be aging-associated diseases (diabetes, hypertension, and cardiovascular and cerebrovascular diseases), exhibit increased susceptibility [5]. Moreover, the spread of SARS-CoV-2 as well as severe acute respiratory syndrome coronavirus (SARS-CoV) in 2003 made it clear that these aging patients are more likely to progress to severe disease and die more easily from these infections than younger people [6-8]. After analyzing the data for 1099 COVID-19 patients from 552 hospitals in China, Nanshan Zhong et al. found that patients with severe disease were older than those with nonsevere disease and that coexisting illness was more common among patients in the severe group[9]. In the United States, 80% of deaths have occurred in patients over the age of 65 years, and patients aged 85 years and over have a high proportion of severe outcomes, mirroring the experience in China [10]. According to a meta-analysis, serious aging-related chronic diseases(associated with a pathological role of cellular senescence), including hypertension, diabetes, chronic obstructive pulmonary disease (COPD), cardiovascular disease, and cerebrovascular disease, are independent risk factors associated with COVID-19 patients [11]. ...
SARS-CoV-2 and COVID-19 in older adults: what we may expect regarding pathogenesis, immune responses, and outcomes
2
2020
... New coronavirus-exposed populations are generally susceptible, but elderly people, especially those with underlying conditions normally considered to be aging-associated diseases (diabetes, hypertension, and cardiovascular and cerebrovascular diseases), exhibit increased susceptibility [5]. Moreover, the spread of SARS-CoV-2 as well as severe acute respiratory syndrome coronavirus (SARS-CoV) in 2003 made it clear that these aging patients are more likely to progress to severe disease and die more easily from these infections than younger people [6-8]. After analyzing the data for 1099 COVID-19 patients from 552 hospitals in China, Nanshan Zhong et al. found that patients with severe disease were older than those with nonsevere disease and that coexisting illness was more common among patients in the severe group[9]. In the United States, 80% of deaths have occurred in patients over the age of 65 years, and patients aged 85 years and over have a high proportion of severe outcomes, mirroring the experience in China [10]. According to a meta-analysis, serious aging-related chronic diseases(associated with a pathological role of cellular senescence), including hypertension, diabetes, chronic obstructive pulmonary disease (COPD), cardiovascular disease, and cerebrovascular disease, are independent risk factors associated with COVID-19 patients [11]. ...
... Current evidence suggests that elderly patients with past comorbidities or dyspnea should be closely monitored for signs of disease progression, decompensation, and exacerbation of illness, especially 1-2 weeks after the onset of symptoms[10, 67]. Presently, there are no officially approved medicines available against SARS-CoV-2. Although the management of COVID-19 patients is primarily supportive, specific therapies are still under investigation. These therapies include current and potential antiviral drugs, anti-senescence drugs, immunosuppressive agents, steroids, mesenchymal stem cell (MSC) transplantation, and an artificial liver system (ALS), among others (Table 1). In the following paragraphs, we aim to highlight the proposed therapeutic strategies [68]. ...
Does comorbidity increase the risk of patients with COVID-19: evidence from meta-analysis
2
2020
... New coronavirus-exposed populations are generally susceptible, but elderly people, especially those with underlying conditions normally considered to be aging-associated diseases (diabetes, hypertension, and cardiovascular and cerebrovascular diseases), exhibit increased susceptibility [5]. Moreover, the spread of SARS-CoV-2 as well as severe acute respiratory syndrome coronavirus (SARS-CoV) in 2003 made it clear that these aging patients are more likely to progress to severe disease and die more easily from these infections than younger people [6-8]. After analyzing the data for 1099 COVID-19 patients from 552 hospitals in China, Nanshan Zhong et al. found that patients with severe disease were older than those with nonsevere disease and that coexisting illness was more common among patients in the severe group[9]. In the United States, 80% of deaths have occurred in patients over the age of 65 years, and patients aged 85 years and over have a high proportion of severe outcomes, mirroring the experience in China [10]. According to a meta-analysis, serious aging-related chronic diseases(associated with a pathological role of cellular senescence), including hypertension, diabetes, chronic obstructive pulmonary disease (COPD), cardiovascular disease, and cerebrovascular disease, are independent risk factors associated with COVID-19 patients [11]. ...
... ACE2 is enriched in the heart and plays an essential role in the regulation of heart function [36]. Burrell et al. indicated that ACE2 expression is increased in myocardial infarction in humans and rats [37]. Chen et al. performed state-of-the-art single-cell atlas analysis of the adult human heart and revealed pericytes with high expression levels of ACE2 as target cells of SARS-CoV-2. Patients with coronary heart disease (CHD) showed increased ACE2expression at the mRNA and protein levels [38]. Patients with CHD and infected with SARS-CoV-2 are at an elevated risk of progressing into severe disease [11, 29]. Conversely, acute cardiac injury is reported as one of the most common complications in COVID-19 patients, which significantly exacerbates disease severity [39]. This evidence suggests that enrichment of ACE2 in the myocardium makes the heart one of the main target organs for SARS-CoV-2 infection. The expression level of ACE2 in cardiomyocytes is closely related to the poor prognosis of COVID-19 patients with heart diseases and the severity of COVID-19-induced heart injury. ...
Risk factors for disease severity, unimprovement, and mortality in COVID-19 patients in Wuhan, China
2
2020
... Similar to those in younger patients, fever, cough and sputum are the most common early symptoms in elderly patients. Elderly patients are more likely to have severe COVID-19 conditions, show lack of improvement, and die [12]. Analyzing a total of 56 COVID-19 patients, Liu et al. found that the pneumonia severity index (PSI) score of elderly patients was higher than that of young and middle-aged patients. The proportion of patients with PSI grades IV and V was significantly higher in elderly patients [13]. The incidence of the common fatal presentations of COVID-19 (including ARDS, shock, arrhythmia and acute cardiac injury) in elderly patients is higher than in young patients [12, 14, 15]. Wang et al. included patients with laboratory-confirmed COVID-19 and ascurtained the viral load by reverse transcriptase quantitative PCR (RT-qPCR). The results showed that older age was correlated with higher SARS-CoV-2 load [16]. Studies of SARS-CoV have shown that a high initial viral load is associated with death [17]. Accumulating evidence indicates that the SARS-CoV-2 viral load correlates with the risk of COVID-19 progression and poor prognosis [18, 19]. Thus, it is conceivable that the poor prognosis of elderly COVID-19 patients may be related to a higher viral load. However, the underlying mechanism requires further exploration. ...
... ]. The incidence of the common fatal presentations of COVID-19 (including ARDS, shock, arrhythmia and acute cardiac injury) in elderly patients is higher than in young patients [12, 14, 15]. Wang et al. included patients with laboratory-confirmed COVID-19 and ascurtained the viral load by reverse transcriptase quantitative PCR (RT-qPCR). The results showed that older age was correlated with higher SARS-CoV-2 load [16]. Studies of SARS-CoV have shown that a high initial viral load is associated with death [17]. Accumulating evidence indicates that the SARS-CoV-2 viral load correlates with the risk of COVID-19 progression and poor prognosis [18, 19]. Thus, it is conceivable that the poor prognosis of elderly COVID-19 patients may be related to a higher viral load. However, the underlying mechanism requires further exploration. ...
Clinical features of COVID-19 in elderly patients: A comparison with young and middle-aged patients
1
2020
... Similar to those in younger patients, fever, cough and sputum are the most common early symptoms in elderly patients. Elderly patients are more likely to have severe COVID-19 conditions, show lack of improvement, and die [12]. Analyzing a total of 56 COVID-19 patients, Liu et al. found that the pneumonia severity index (PSI) score of elderly patients was higher than that of young and middle-aged patients. The proportion of patients with PSI grades IV and V was significantly higher in elderly patients [13]. The incidence of the common fatal presentations of COVID-19 (including ARDS, shock, arrhythmia and acute cardiac injury) in elderly patients is higher than in young patients [12, 14, 15]. Wang et al. included patients with laboratory-confirmed COVID-19 and ascurtained the viral load by reverse transcriptase quantitative PCR (RT-qPCR). The results showed that older age was correlated with higher SARS-CoV-2 load [16]. Studies of SARS-CoV have shown that a high initial viral load is associated with death [17]. Accumulating evidence indicates that the SARS-CoV-2 viral load correlates with the risk of COVID-19 progression and poor prognosis [18, 19]. Thus, it is conceivable that the poor prognosis of elderly COVID-19 patients may be related to a higher viral load. However, the underlying mechanism requires further exploration. ...
Clinical characteristics and outcomes of patients undergoing surgeries during the incubation period of COVID-19 infection
1
2020
... Similar to those in younger patients, fever, cough and sputum are the most common early symptoms in elderly patients. Elderly patients are more likely to have severe COVID-19 conditions, show lack of improvement, and die [12]. Analyzing a total of 56 COVID-19 patients, Liu et al. found that the pneumonia severity index (PSI) score of elderly patients was higher than that of young and middle-aged patients. The proportion of patients with PSI grades IV and V was significantly higher in elderly patients [13]. The incidence of the common fatal presentations of COVID-19 (including ARDS, shock, arrhythmia and acute cardiac injury) in elderly patients is higher than in young patients [12, 14, 15]. Wang et al. included patients with laboratory-confirmed COVID-19 and ascurtained the viral load by reverse transcriptase quantitative PCR (RT-qPCR). The results showed that older age was correlated with higher SARS-CoV-2 load [16]. Studies of SARS-CoV have shown that a high initial viral load is associated with death [17]. Accumulating evidence indicates that the SARS-CoV-2 viral load correlates with the risk of COVID-19 progression and poor prognosis [18, 19]. Thus, it is conceivable that the poor prognosis of elderly COVID-19 patients may be related to a higher viral load. However, the underlying mechanism requires further exploration. ...
Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China
1
2020
... Similar to those in younger patients, fever, cough and sputum are the most common early symptoms in elderly patients. Elderly patients are more likely to have severe COVID-19 conditions, show lack of improvement, and die [12]. Analyzing a total of 56 COVID-19 patients, Liu et al. found that the pneumonia severity index (PSI) score of elderly patients was higher than that of young and middle-aged patients. The proportion of patients with PSI grades IV and V was significantly higher in elderly patients [13]. The incidence of the common fatal presentations of COVID-19 (including ARDS, shock, arrhythmia and acute cardiac injury) in elderly patients is higher than in young patients [12, 14, 15]. Wang et al. included patients with laboratory-confirmed COVID-19 and ascurtained the viral load by reverse transcriptase quantitative PCR (RT-qPCR). The results showed that older age was correlated with higher SARS-CoV-2 load [16]. Studies of SARS-CoV have shown that a high initial viral load is associated with death [17]. Accumulating evidence indicates that the SARS-CoV-2 viral load correlates with the risk of COVID-19 progression and poor prognosis [18, 19]. Thus, it is conceivable that the poor prognosis of elderly COVID-19 patients may be related to a higher viral load. However, the underlying mechanism requires further exploration. ...
Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: an observational cohort study
1
2020
... Similar to those in younger patients, fever, cough and sputum are the most common early symptoms in elderly patients. Elderly patients are more likely to have severe COVID-19 conditions, show lack of improvement, and die [12]. Analyzing a total of 56 COVID-19 patients, Liu et al. found that the pneumonia severity index (PSI) score of elderly patients was higher than that of young and middle-aged patients. The proportion of patients with PSI grades IV and V was significantly higher in elderly patients [13]. The incidence of the common fatal presentations of COVID-19 (including ARDS, shock, arrhythmia and acute cardiac injury) in elderly patients is higher than in young patients [12, 14, 15]. Wang et al. included patients with laboratory-confirmed COVID-19 and ascurtained the viral load by reverse transcriptase quantitative PCR (RT-qPCR). The results showed that older age was correlated with higher SARS-CoV-2 load [16]. Studies of SARS-CoV have shown that a high initial viral load is associated with death [17]. Accumulating evidence indicates that the SARS-CoV-2 viral load correlates with the risk of COVID-19 progression and poor prognosis [18, 19]. Thus, it is conceivable that the poor prognosis of elderly COVID-19 patients may be related to a higher viral load. However, the underlying mechanism requires further exploration. ...
Initial viral load and the outcomes of SARS
1
2004
... Similar to those in younger patients, fever, cough and sputum are the most common early symptoms in elderly patients. Elderly patients are more likely to have severe COVID-19 conditions, show lack of improvement, and die [12]. Analyzing a total of 56 COVID-19 patients, Liu et al. found that the pneumonia severity index (PSI) score of elderly patients was higher than that of young and middle-aged patients. The proportion of patients with PSI grades IV and V was significantly higher in elderly patients [13]. The incidence of the common fatal presentations of COVID-19 (including ARDS, shock, arrhythmia and acute cardiac injury) in elderly patients is higher than in young patients [12, 14, 15]. Wang et al. included patients with laboratory-confirmed COVID-19 and ascurtained the viral load by reverse transcriptase quantitative PCR (RT-qPCR). The results showed that older age was correlated with higher SARS-CoV-2 load [16]. Studies of SARS-CoV have shown that a high initial viral load is associated with death [17]. Accumulating evidence indicates that the SARS-CoV-2 viral load correlates with the risk of COVID-19 progression and poor prognosis [18, 19]. Thus, it is conceivable that the poor prognosis of elderly COVID-19 patients may be related to a higher viral load. However, the underlying mechanism requires further exploration. ...
SARS-CoV-2 viral load in sputum correlates with risk of COVID-19 progression
1
2020
... Similar to those in younger patients, fever, cough and sputum are the most common early symptoms in elderly patients. Elderly patients are more likely to have severe COVID-19 conditions, show lack of improvement, and die [12]. Analyzing a total of 56 COVID-19 patients, Liu et al. found that the pneumonia severity index (PSI) score of elderly patients was higher than that of young and middle-aged patients. The proportion of patients with PSI grades IV and V was significantly higher in elderly patients [13]. The incidence of the common fatal presentations of COVID-19 (including ARDS, shock, arrhythmia and acute cardiac injury) in elderly patients is higher than in young patients [12, 14, 15]. Wang et al. included patients with laboratory-confirmed COVID-19 and ascurtained the viral load by reverse transcriptase quantitative PCR (RT-qPCR). The results showed that older age was correlated with higher SARS-CoV-2 load [16]. Studies of SARS-CoV have shown that a high initial viral load is associated with death [17]. Accumulating evidence indicates that the SARS-CoV-2 viral load correlates with the risk of COVID-19 progression and poor prognosis [18, 19]. Thus, it is conceivable that the poor prognosis of elderly COVID-19 patients may be related to a higher viral load. However, the underlying mechanism requires further exploration. ...
Viral load dynamics and disease severity in patients infected with SARS-CoV-2 in Zhejiang province, China, January-March 2020: retrospective cohort study
1
2020
... Similar to those in younger patients, fever, cough and sputum are the most common early symptoms in elderly patients. Elderly patients are more likely to have severe COVID-19 conditions, show lack of improvement, and die [12]. Analyzing a total of 56 COVID-19 patients, Liu et al. found that the pneumonia severity index (PSI) score of elderly patients was higher than that of young and middle-aged patients. The proportion of patients with PSI grades IV and V was significantly higher in elderly patients [13]. The incidence of the common fatal presentations of COVID-19 (including ARDS, shock, arrhythmia and acute cardiac injury) in elderly patients is higher than in young patients [12, 14, 15]. Wang et al. included patients with laboratory-confirmed COVID-19 and ascurtained the viral load by reverse transcriptase quantitative PCR (RT-qPCR). The results showed that older age was correlated with higher SARS-CoV-2 load [16]. Studies of SARS-CoV have shown that a high initial viral load is associated with death [17]. Accumulating evidence indicates that the SARS-CoV-2 viral load correlates with the risk of COVID-19 progression and poor prognosis [18, 19]. Thus, it is conceivable that the poor prognosis of elderly COVID-19 patients may be related to a higher viral load. However, the underlying mechanism requires further exploration. ...
Tissue specificity of senescent cell accumulation during physiologic and accelerated aging of mice
1
2020
... Senescent cells accumulate with age in vertebrates and promote aging mainly through the senescence-associated secretory phenotype (SASP) [20]. Data have shown that RNA viruses, such as influenza virus, display enhanced replication efficiency in senescent cells, which suggests that the accumulation of senescent cells in aging and age-related diseases may play a role in this phenomenon. However, the response to SARS-COV-2 that occurs in senescent cells is still poorly understood [8]. ...
A pneumonia outbreak associated with a new coronavirus of probable bat origin
1
2020
... Angiotensin-converting enzyme 2 (ACE2) has been identified as areceptor for SARS-CoV-2, which directly interacts with COVID-19 spike(S) glycoproteins [21, 22]. During infection, the S protein is cleaved into S1 andS2 by the host transmembrane protease/serine subfamily member 2 (TMPRSS2)and protease furin [23].S1 directly binds to ACE2 and S2 plays a role in membrane fusion [24]. Zhou et al. analysed the expression of ACE2, together withTMPRSS2 and Furin by the method of single-cell RNA profiling combined with the protein information in different tissues. According to the rank list of candidate cells potentially vulnerable to SARS-CoV-2,the top targets were lung alveolar type 2 (AT2) cells and macrophages, followed by cardiomyocytes and adrenal gland stromal cells [25]. These findings were consistent with prominent lung symptoms, frequent heart damage and rare bowel symptoms. Cluster of differentiation 26 (CD26) is also recommended as a potential receptor for SARS-COV-2 [22, 26]. Intriguingly, both ACE2 and CD26 show associations with senescence and immunoregulation. ...
COVID-19 and comorbidities: A role for dipeptidyl peptidase 4 (DPP4) in disease severity?
3
2020
... Angiotensin-converting enzyme 2 (ACE2) has been identified as areceptor for SARS-CoV-2, which directly interacts with COVID-19 spike(S) glycoproteins [21, 22]. During infection, the S protein is cleaved into S1 andS2 by the host transmembrane protease/serine subfamily member 2 (TMPRSS2)and protease furin [23].S1 directly binds to ACE2 and S2 plays a role in membrane fusion [24]. Zhou et al. analysed the expression of ACE2, together withTMPRSS2 and Furin by the method of single-cell RNA profiling combined with the protein information in different tissues. According to the rank list of candidate cells potentially vulnerable to SARS-CoV-2,the top targets were lung alveolar type 2 (AT2) cells and macrophages, followed by cardiomyocytes and adrenal gland stromal cells [25]. These findings were consistent with prominent lung symptoms, frequent heart damage and rare bowel symptoms. Cluster of differentiation 26 (CD26) is also recommended as a potential receptor for SARS-COV-2 [22, 26]. Intriguingly, both ACE2 and CD26 show associations with senescence and immunoregulation. ...
... ]. These findings were consistent with prominent lung symptoms, frequent heart damage and rare bowel symptoms. Cluster of differentiation 26 (CD26) is also recommended as a potential receptor for SARS-COV-2 [22, 26]. Intriguingly, both ACE2 and CD26 show associations with senescence and immunoregulation. ...
... CD26, also known as dipeptidyl peptidase 4 (DPP4), is a serine exopeptidase that is expressed ubiquitously in human tissues, including lung, kidney, liver, gut, and immune cell s(including T-cells, activated B-cells, activated natural killer cells and myeloid cells) [52, 53]. CD26 plays multiple roles in nutrition, metabolism, and the immune and endocrine systems. Using mass spectrometry analysis, Kim et al. identified CD26 as a surface protein that is expressed at significantly higher levels in senescent cells. CD26 activity is higher in older than in younger individuals [54]. Overly upregulated CD26 expression and activity are associated with diabetes, obesity and metabolic syndrome, which are reported to influence COVID-19 severity [22, 55]. ...
Structural features of coronavirus SARS-CoV-2 spike protein: Targets for vaccination
1
2020
... Angiotensin-converting enzyme 2 (ACE2) has been identified as areceptor for SARS-CoV-2, which directly interacts with COVID-19 spike(S) glycoproteins [21, 22]. During infection, the S protein is cleaved into S1 andS2 by the host transmembrane protease/serine subfamily member 2 (TMPRSS2)and protease furin [23].S1 directly binds to ACE2 and S2 plays a role in membrane fusion [24]. Zhou et al. analysed the expression of ACE2, together withTMPRSS2 and Furin by the method of single-cell RNA profiling combined with the protein information in different tissues. According to the rank list of candidate cells potentially vulnerable to SARS-CoV-2,the top targets were lung alveolar type 2 (AT2) cells and macrophages, followed by cardiomyocytes and adrenal gland stromal cells [25]. These findings were consistent with prominent lung symptoms, frequent heart damage and rare bowel symptoms. Cluster of differentiation 26 (CD26) is also recommended as a potential receptor for SARS-COV-2 [22, 26]. Intriguingly, both ACE2 and CD26 show associations with senescence and immunoregulation. ...
Inhibition of SARS-CoV-2 entry through the ACE2/TMPRSS2 pathway: a promising approach for uncovering early COVID-19 drug therapies
1
2020
... Angiotensin-converting enzyme 2 (ACE2) has been identified as areceptor for SARS-CoV-2, which directly interacts with COVID-19 spike(S) glycoproteins [21, 22]. During infection, the S protein is cleaved into S1 andS2 by the host transmembrane protease/serine subfamily member 2 (TMPRSS2)and protease furin [23].S1 directly binds to ACE2 and S2 plays a role in membrane fusion [24]. Zhou et al. analysed the expression of ACE2, together withTMPRSS2 and Furin by the method of single-cell RNA profiling combined with the protein information in different tissues. According to the rank list of candidate cells potentially vulnerable to SARS-CoV-2,the top targets were lung alveolar type 2 (AT2) cells and macrophages, followed by cardiomyocytes and adrenal gland stromal cells [25]. These findings were consistent with prominent lung symptoms, frequent heart damage and rare bowel symptoms. Cluster of differentiation 26 (CD26) is also recommended as a potential receptor for SARS-COV-2 [22, 26]. Intriguingly, both ACE2 and CD26 show associations with senescence and immunoregulation. ...
Systemic analysis of tissue cells potentially vulnerable to SARS-CoV-2 infection by the protein-proofed single-cell RNA profiling of ACE2, TMPRSS2 and Furin proteases
1
2020
... Angiotensin-converting enzyme 2 (ACE2) has been identified as areceptor for SARS-CoV-2, which directly interacts with COVID-19 spike(S) glycoproteins [21, 22]. During infection, the S protein is cleaved into S1 andS2 by the host transmembrane protease/serine subfamily member 2 (TMPRSS2)and protease furin [23].S1 directly binds to ACE2 and S2 plays a role in membrane fusion [24]. Zhou et al. analysed the expression of ACE2, together withTMPRSS2 and Furin by the method of single-cell RNA profiling combined with the protein information in different tissues. According to the rank list of candidate cells potentially vulnerable to SARS-CoV-2,the top targets were lung alveolar type 2 (AT2) cells and macrophages, followed by cardiomyocytes and adrenal gland stromal cells [25]. These findings were consistent with prominent lung symptoms, frequent heart damage and rare bowel symptoms. Cluster of differentiation 26 (CD26) is also recommended as a potential receptor for SARS-COV-2 [22, 26]. Intriguingly, both ACE2 and CD26 show associations with senescence and immunoregulation. ...
Emerging WuHan (COVID-19) coronavirus: glycan shield and structure prediction of spike glycoprotein and its interaction with human CD26
1
2020
... Angiotensin-converting enzyme 2 (ACE2) has been identified as areceptor for SARS-CoV-2, which directly interacts with COVID-19 spike(S) glycoproteins [21, 22]. During infection, the S protein is cleaved into S1 andS2 by the host transmembrane protease/serine subfamily member 2 (TMPRSS2)and protease furin [23].S1 directly binds to ACE2 and S2 plays a role in membrane fusion [24]. Zhou et al. analysed the expression of ACE2, together withTMPRSS2 and Furin by the method of single-cell RNA profiling combined with the protein information in different tissues. According to the rank list of candidate cells potentially vulnerable to SARS-CoV-2,the top targets were lung alveolar type 2 (AT2) cells and macrophages, followed by cardiomyocytes and adrenal gland stromal cells [25]. These findings were consistent with prominent lung symptoms, frequent heart damage and rare bowel symptoms. Cluster of differentiation 26 (CD26) is also recommended as a potential receptor for SARS-COV-2 [22, 26]. Intriguingly, both ACE2 and CD26 show associations with senescence and immunoregulation. ...
Renin-angiotensin-aldosterone (RAAS): The ubiquitous system for homeostasis and pathologies
1
2017
... ACE2, which is widely distributed in the heart, kidneys, lungs, liver, intestine, brain and testes, is a known crucial component of the renin-angiotensin system (RAS)[27]. According to Khemais-Benkhiat et al., RAS is upregulated in endothelial cells with premature and replicative senescence [28]. It has been suggested that differential levels of ACE2 in human organs, especially the cardiac and pulmonary tissues of younger versus older adults, may be responsible for the disease virulence spectrum observed in COVID-19 patients [29]. Ziegler et al. discovered that ACE2 was a human interferon-stimulated gene in airway epithelial cells. SARS-CoV-2 could enhance infection through species-specific interferon-driven upregulation of ACE2 [30]. Smith et al. also identified ACE2 as an interferon-stimulated gene in lung cells. They found that chronic smoke exposure and inflammatory signaling could increase ACE2 expression levels in the respiratory tract. Their findings suggested that SARS-CoV-2 infections could create positive feedback loops that increase ACE2 expression and promote viral dissemination [31]. ...
The Redox-sensitive Induction of the Local Angiotensin System Promotes Both Premature and Replicative Endothelial Senescence: Preventive Effect of a Standardized Crataegus Extract
1
2016
... ACE2, which is widely distributed in the heart, kidneys, lungs, liver, intestine, brain and testes, is a known crucial component of the renin-angiotensin system (RAS)[27]. According to Khemais-Benkhiat et al., RAS is upregulated in endothelial cells with premature and replicative senescence [28]. It has been suggested that differential levels of ACE2 in human organs, especially the cardiac and pulmonary tissues of younger versus older adults, may be responsible for the disease virulence spectrum observed in COVID-19 patients [29]. Ziegler et al. discovered that ACE2 was a human interferon-stimulated gene in airway epithelial cells. SARS-CoV-2 could enhance infection through species-specific interferon-driven upregulation of ACE2 [30]. Smith et al. also identified ACE2 as an interferon-stimulated gene in lung cells. They found that chronic smoke exposure and inflammatory signaling could increase ACE2 expression levels in the respiratory tract. Their findings suggested that SARS-CoV-2 infections could create positive feedback loops that increase ACE2 expression and promote viral dissemination [31]. ...
Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China
2
2020
... ACE2, which is widely distributed in the heart, kidneys, lungs, liver, intestine, brain and testes, is a known crucial component of the renin-angiotensin system (RAS)[27]. According to Khemais-Benkhiat et al., RAS is upregulated in endothelial cells with premature and replicative senescence [28]. It has been suggested that differential levels of ACE2 in human organs, especially the cardiac and pulmonary tissues of younger versus older adults, may be responsible for the disease virulence spectrum observed in COVID-19 patients [29]. Ziegler et al. discovered that ACE2 was a human interferon-stimulated gene in airway epithelial cells. SARS-CoV-2 could enhance infection through species-specific interferon-driven upregulation of ACE2 [30]. Smith et al. also identified ACE2 as an interferon-stimulated gene in lung cells. They found that chronic smoke exposure and inflammatory signaling could increase ACE2 expression levels in the respiratory tract. Their findings suggested that SARS-CoV-2 infections could create positive feedback loops that increase ACE2 expression and promote viral dissemination [31]. ...
... ACE2 is enriched in the heart and plays an essential role in the regulation of heart function [36]. Burrell et al. indicated that ACE2 expression is increased in myocardial infarction in humans and rats [37]. Chen et al. performed state-of-the-art single-cell atlas analysis of the adult human heart and revealed pericytes with high expression levels of ACE2 as target cells of SARS-CoV-2. Patients with coronary heart disease (CHD) showed increased ACE2expression at the mRNA and protein levels [38]. Patients with CHD and infected with SARS-CoV-2 are at an elevated risk of progressing into severe disease [11, 29]. Conversely, acute cardiac injury is reported as one of the most common complications in COVID-19 patients, which significantly exacerbates disease severity [39]. This evidence suggests that enrichment of ACE2 in the myocardium makes the heart one of the main target organs for SARS-CoV-2 infection. The expression level of ACE2 in cardiomyocytes is closely related to the poor prognosis of COVID-19 patients with heart diseases and the severity of COVID-19-induced heart injury. ...
SARS-CoV-2 Receptor ACE2 Is an Interferon-Stimulated Gene in Human Airway Epithelial Cells and Is Detected in Specific Cell Subsets across Tissues
1
2020
... ACE2, which is widely distributed in the heart, kidneys, lungs, liver, intestine, brain and testes, is a known crucial component of the renin-angiotensin system (RAS)[27]. According to Khemais-Benkhiat et al., RAS is upregulated in endothelial cells with premature and replicative senescence [28]. It has been suggested that differential levels of ACE2 in human organs, especially the cardiac and pulmonary tissues of younger versus older adults, may be responsible for the disease virulence spectrum observed in COVID-19 patients [29]. Ziegler et al. discovered that ACE2 was a human interferon-stimulated gene in airway epithelial cells. SARS-CoV-2 could enhance infection through species-specific interferon-driven upregulation of ACE2 [30]. Smith et al. also identified ACE2 as an interferon-stimulated gene in lung cells. They found that chronic smoke exposure and inflammatory signaling could increase ACE2 expression levels in the respiratory tract. Their findings suggested that SARS-CoV-2 infections could create positive feedback loops that increase ACE2 expression and promote viral dissemination [31]. ...
Cigarette Smoke Exposure and Inflammatory Signaling Increase the Expression of the SARS-CoV-2 Receptor ACE2 in the Respiratory Tract
1
2020
... ACE2, which is widely distributed in the heart, kidneys, lungs, liver, intestine, brain and testes, is a known crucial component of the renin-angiotensin system (RAS)[27]. According to Khemais-Benkhiat et al., RAS is upregulated in endothelial cells with premature and replicative senescence [28]. It has been suggested that differential levels of ACE2 in human organs, especially the cardiac and pulmonary tissues of younger versus older adults, may be responsible for the disease virulence spectrum observed in COVID-19 patients [29]. Ziegler et al. discovered that ACE2 was a human interferon-stimulated gene in airway epithelial cells. SARS-CoV-2 could enhance infection through species-specific interferon-driven upregulation of ACE2 [30]. Smith et al. also identified ACE2 as an interferon-stimulated gene in lung cells. They found that chronic smoke exposure and inflammatory signaling could increase ACE2 expression levels in the respiratory tract. Their findings suggested that SARS-CoV-2 infections could create positive feedback loops that increase ACE2 expression and promote viral dissemination [31]. ...
Age- and gender-related difference of ACE2 expression in rat lung
1
2006
... Interestingly, it has been previously established that ACE2 shows a protective effect in the lungs and that ACE2 expression in the lungs decreases during aging. The lower ACE2 level in the lungs may contribute to the poor prognosis of SARS in the aged group [32]. According to previous research, following SARS-COV entry, ACE2 expression is downregulated dramatically, which leads to a compensatory overproduction of angiotensin 2 (AngII), therefore increasing lung vascular permeability and aggravating lung failure [33]. A similar phenomenon is also observed in SARS-CoV-2-infected lung tissue [34]. According to Datta et al., SARS-CoV-2infects ACE2-expressing cells in the lung, inducing shedding of ACE2 from the cells and, thus, effectively reducing ACE2 expression levels [35]. These findings support the proposed role of ACE2 downregulation in both the pathogenesis and progression into ARDS in SARS and COVID-19 patients. ...
Angiotensin-converting enzyme 2 protects from severe acute lung failure
1
2005
... Interestingly, it has been previously established that ACE2 shows a protective effect in the lungs and that ACE2 expression in the lungs decreases during aging. The lower ACE2 level in the lungs may contribute to the poor prognosis of SARS in the aged group [32]. According to previous research, following SARS-COV entry, ACE2 expression is downregulated dramatically, which leads to a compensatory overproduction of angiotensin 2 (AngII), therefore increasing lung vascular permeability and aggravating lung failure [33]. A similar phenomenon is also observed in SARS-CoV-2-infected lung tissue [34]. According to Datta et al., SARS-CoV-2infects ACE2-expressing cells in the lung, inducing shedding of ACE2 from the cells and, thus, effectively reducing ACE2 expression levels [35]. These findings support the proposed role of ACE2 downregulation in both the pathogenesis and progression into ARDS in SARS and COVID-19 patients. ...
ACE2 Activators for the Treatment of Covid 19 Patients
3
2020
... Interestingly, it has been previously established that ACE2 shows a protective effect in the lungs and that ACE2 expression in the lungs decreases during aging. The lower ACE2 level in the lungs may contribute to the poor prognosis of SARS in the aged group [32]. According to previous research, following SARS-COV entry, ACE2 expression is downregulated dramatically, which leads to a compensatory overproduction of angiotensin 2 (AngII), therefore increasing lung vascular permeability and aggravating lung failure [33]. A similar phenomenon is also observed in SARS-CoV-2-infected lung tissue [34]. According to Datta et al., SARS-CoV-2infects ACE2-expressing cells in the lung, inducing shedding of ACE2 from the cells and, thus, effectively reducing ACE2 expression levels [35]. These findings support the proposed role of ACE2 downregulation in both the pathogenesis and progression into ARDS in SARS and COVID-19 patients. ...
... Some researchers have suggested that SARS-CoV-2 induces initial damage effects by downregulating ACE2 expression and blocking ACE2-mediated activity and activating ACE2 may be much more efficacious. Accumulating evidence has illustrated that the activation of ACE2 could be a positive treatment method. ACE2 activators are purported to have two therapeutic effects: avoiding the binding of the S protein of SARS-CoV-2 to ACE2 and promoting the protective effects of different organs, preventing lung injury and fibrosis [34, 114, 115].ACE2 activators, such as diminazene aceturate, are recommended for application in COVID-19 patients [34]. ...
... ].ACE2 activators, such as diminazene aceturate, are recommended for application in COVID-19 patients [34]. ...
SARS-CoV-2 pandemic and research gaps: Understanding SARS-CoV-2 interaction with the ACE2 receptor and implications for therapy
1
2020
... Interestingly, it has been previously established that ACE2 shows a protective effect in the lungs and that ACE2 expression in the lungs decreases during aging. The lower ACE2 level in the lungs may contribute to the poor prognosis of SARS in the aged group [32]. According to previous research, following SARS-COV entry, ACE2 expression is downregulated dramatically, which leads to a compensatory overproduction of angiotensin 2 (AngII), therefore increasing lung vascular permeability and aggravating lung failure [33]. A similar phenomenon is also observed in SARS-CoV-2-infected lung tissue [34]. According to Datta et al., SARS-CoV-2infects ACE2-expressing cells in the lung, inducing shedding of ACE2 from the cells and, thus, effectively reducing ACE2 expression levels [35]. These findings support the proposed role of ACE2 downregulation in both the pathogenesis and progression into ARDS in SARS and COVID-19 patients. ...
Angiotensin-converting enzyme 2 is an essential regulator of heart function
1
2002
... ACE2 is enriched in the heart and plays an essential role in the regulation of heart function [36]. Burrell et al. indicated that ACE2 expression is increased in myocardial infarction in humans and rats [37]. Chen et al. performed state-of-the-art single-cell atlas analysis of the adult human heart and revealed pericytes with high expression levels of ACE2 as target cells of SARS-CoV-2. Patients with coronary heart disease (CHD) showed increased ACE2expression at the mRNA and protein levels [38]. Patients with CHD and infected with SARS-CoV-2 are at an elevated risk of progressing into severe disease [11, 29]. Conversely, acute cardiac injury is reported as one of the most common complications in COVID-19 patients, which significantly exacerbates disease severity [39]. This evidence suggests that enrichment of ACE2 in the myocardium makes the heart one of the main target organs for SARS-CoV-2 infection. The expression level of ACE2 in cardiomyocytes is closely related to the poor prognosis of COVID-19 patients with heart diseases and the severity of COVID-19-induced heart injury. ...
Myocardial infarction increases ACE2 expression in rat and humans
1
2005
... ACE2 is enriched in the heart and plays an essential role in the regulation of heart function [36]. Burrell et al. indicated that ACE2 expression is increased in myocardial infarction in humans and rats [37]. Chen et al. performed state-of-the-art single-cell atlas analysis of the adult human heart and revealed pericytes with high expression levels of ACE2 as target cells of SARS-CoV-2. Patients with coronary heart disease (CHD) showed increased ACE2expression at the mRNA and protein levels [38]. Patients with CHD and infected with SARS-CoV-2 are at an elevated risk of progressing into severe disease [11, 29]. Conversely, acute cardiac injury is reported as one of the most common complications in COVID-19 patients, which significantly exacerbates disease severity [39]. This evidence suggests that enrichment of ACE2 in the myocardium makes the heart one of the main target organs for SARS-CoV-2 infection. The expression level of ACE2 in cardiomyocytes is closely related to the poor prognosis of COVID-19 patients with heart diseases and the severity of COVID-19-induced heart injury. ...
The ACE2 expression in human heart indicates new potential mechanism of heart injury among patients infected with SARS-CoV-2
1
2020
... ACE2 is enriched in the heart and plays an essential role in the regulation of heart function [36]. Burrell et al. indicated that ACE2 expression is increased in myocardial infarction in humans and rats [37]. Chen et al. performed state-of-the-art single-cell atlas analysis of the adult human heart and revealed pericytes with high expression levels of ACE2 as target cells of SARS-CoV-2. Patients with coronary heart disease (CHD) showed increased ACE2expression at the mRNA and protein levels [38]. Patients with CHD and infected with SARS-CoV-2 are at an elevated risk of progressing into severe disease [11, 29]. Conversely, acute cardiac injury is reported as one of the most common complications in COVID-19 patients, which significantly exacerbates disease severity [39]. This evidence suggests that enrichment of ACE2 in the myocardium makes the heart one of the main target organs for SARS-CoV-2 infection. The expression level of ACE2 in cardiomyocytes is closely related to the poor prognosis of COVID-19 patients with heart diseases and the severity of COVID-19-induced heart injury. ...
Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China
1
2020
... ACE2 is enriched in the heart and plays an essential role in the regulation of heart function [36]. Burrell et al. indicated that ACE2 expression is increased in myocardial infarction in humans and rats [37]. Chen et al. performed state-of-the-art single-cell atlas analysis of the adult human heart and revealed pericytes with high expression levels of ACE2 as target cells of SARS-CoV-2. Patients with coronary heart disease (CHD) showed increased ACE2expression at the mRNA and protein levels [38]. Patients with CHD and infected with SARS-CoV-2 are at an elevated risk of progressing into severe disease [11, 29]. Conversely, acute cardiac injury is reported as one of the most common complications in COVID-19 patients, which significantly exacerbates disease severity [39]. This evidence suggests that enrichment of ACE2 in the myocardium makes the heart one of the main target organs for SARS-CoV-2 infection. The expression level of ACE2 in cardiomyocytes is closely related to the poor prognosis of COVID-19 patients with heart diseases and the severity of COVID-19-induced heart injury. ...
The Serum Profile of Hypercytokinemia Factors Identified in H7N9-Infected Patients can Predict Fatal Outcomes
1
2015
... Cytokine storms, namely, hypercytokinemia, a frequent feature of severe SARS, MERS, H5N1 influenza and H7N9 influenza, are associated with disease severity and are a predictor of prognosis [40-42]. Accumulating data suggest that depletion of lymphocytes, activation of cytotoxic T-lymphocytes, neutrophils and neutrophil-mediated cytokine storms may play key roles in COVID-19 pathogenesis [43]. COVID-19 results in increased levels of plasma cytokines, including interleukin-6 (IL-6), interleukin-1β (IL-1β), interleukin-7 (IL-7), interleukin-8 (IL-8), interleukin-9 (IL-9), interleukin-10 (IL-10), granulocyte colony stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), interferon-γ (IFN-γ), tumor necrosis factor (TNF-α) and vascular endothelial growth factor A (VEGFA). ICU patients with COVID-19 produced higher levels of IL-6 than those not requiring ICU care [44]. According to a meta-analysis, mean IL-6 serum levels are2.9 times higher in patients with severe disease than in those with nonsevere disease [45]. HighIL-6 levels are closely correlated with the serum SARS-CoV-2 viral load, which further affects vital signs and the occurrence of ARDS inCOVID-19 patients [46]. Moreover, as a mediator of SASP, IL-6 is the main functional marker of cell aging [5, 47], and the increase in IL-6 content may correspond to the age-dependent increase in mortality of COVID-19 patients [48]. ...
Fatal outcome of human influenza A (H5N1) is associated with high viral load and hypercytokinemia
0
2006
MERS-CoV infection in humans is associated with a pro-inflammatory Th1 and Th17 cytokine profile
1
2018
... Cytokine storms, namely, hypercytokinemia, a frequent feature of severe SARS, MERS, H5N1 influenza and H7N9 influenza, are associated with disease severity and are a predictor of prognosis [40-42]. Accumulating data suggest that depletion of lymphocytes, activation of cytotoxic T-lymphocytes, neutrophils and neutrophil-mediated cytokine storms may play key roles in COVID-19 pathogenesis [43]. COVID-19 results in increased levels of plasma cytokines, including interleukin-6 (IL-6), interleukin-1β (IL-1β), interleukin-7 (IL-7), interleukin-8 (IL-8), interleukin-9 (IL-9), interleukin-10 (IL-10), granulocyte colony stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), interferon-γ (IFN-γ), tumor necrosis factor (TNF-α) and vascular endothelial growth factor A (VEGFA). ICU patients with COVID-19 produced higher levels of IL-6 than those not requiring ICU care [44]. According to a meta-analysis, mean IL-6 serum levels are2.9 times higher in patients with severe disease than in those with nonsevere disease [45]. HighIL-6 levels are closely correlated with the serum SARS-CoV-2 viral load, which further affects vital signs and the occurrence of ARDS inCOVID-19 patients [46]. Moreover, as a mediator of SASP, IL-6 is the main functional marker of cell aging [5, 47], and the increase in IL-6 content may correspond to the age-dependent increase in mortality of COVID-19 patients [48]. ...
A glimpse into the eye of the COVID-19 cytokine storm
1
2020
... Cytokine storms, namely, hypercytokinemia, a frequent feature of severe SARS, MERS, H5N1 influenza and H7N9 influenza, are associated with disease severity and are a predictor of prognosis [40-42]. Accumulating data suggest that depletion of lymphocytes, activation of cytotoxic T-lymphocytes, neutrophils and neutrophil-mediated cytokine storms may play key roles in COVID-19 pathogenesis [43]. COVID-19 results in increased levels of plasma cytokines, including interleukin-6 (IL-6), interleukin-1β (IL-1β), interleukin-7 (IL-7), interleukin-8 (IL-8), interleukin-9 (IL-9), interleukin-10 (IL-10), granulocyte colony stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), interferon-γ (IFN-γ), tumor necrosis factor (TNF-α) and vascular endothelial growth factor A (VEGFA). ICU patients with COVID-19 produced higher levels of IL-6 than those not requiring ICU care [44]. According to a meta-analysis, mean IL-6 serum levels are2.9 times higher in patients with severe disease than in those with nonsevere disease [45]. HighIL-6 levels are closely correlated with the serum SARS-CoV-2 viral load, which further affects vital signs and the occurrence of ARDS inCOVID-19 patients [46]. Moreover, as a mediator of SASP, IL-6 is the main functional marker of cell aging [5, 47], and the increase in IL-6 content may correspond to the age-dependent increase in mortality of COVID-19 patients [48]. ...
The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak
1
2020
... Cytokine storms, namely, hypercytokinemia, a frequent feature of severe SARS, MERS, H5N1 influenza and H7N9 influenza, are associated with disease severity and are a predictor of prognosis [40-42]. Accumulating data suggest that depletion of lymphocytes, activation of cytotoxic T-lymphocytes, neutrophils and neutrophil-mediated cytokine storms may play key roles in COVID-19 pathogenesis [43]. COVID-19 results in increased levels of plasma cytokines, including interleukin-6 (IL-6), interleukin-1β (IL-1β), interleukin-7 (IL-7), interleukin-8 (IL-8), interleukin-9 (IL-9), interleukin-10 (IL-10), granulocyte colony stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), interferon-γ (IFN-γ), tumor necrosis factor (TNF-α) and vascular endothelial growth factor A (VEGFA). ICU patients with COVID-19 produced higher levels of IL-6 than those not requiring ICU care [44]. According to a meta-analysis, mean IL-6 serum levels are2.9 times higher in patients with severe disease than in those with nonsevere disease [45]. HighIL-6 levels are closely correlated with the serum SARS-CoV-2 viral load, which further affects vital signs and the occurrence of ARDS inCOVID-19 patients [46]. Moreover, as a mediator of SASP, IL-6 is the main functional marker of cell aging [5, 47], and the increase in IL-6 content may correspond to the age-dependent increase in mortality of COVID-19 patients [48]. ...
Elevated Interleukin-6 and Severe COVID-19: A Meta-Analysis
1
2020
... Cytokine storms, namely, hypercytokinemia, a frequent feature of severe SARS, MERS, H5N1 influenza and H7N9 influenza, are associated with disease severity and are a predictor of prognosis [40-42]. Accumulating data suggest that depletion of lymphocytes, activation of cytotoxic T-lymphocytes, neutrophils and neutrophil-mediated cytokine storms may play key roles in COVID-19 pathogenesis [43]. COVID-19 results in increased levels of plasma cytokines, including interleukin-6 (IL-6), interleukin-1β (IL-1β), interleukin-7 (IL-7), interleukin-8 (IL-8), interleukin-9 (IL-9), interleukin-10 (IL-10), granulocyte colony stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), interferon-γ (IFN-γ), tumor necrosis factor (TNF-α) and vascular endothelial growth factor A (VEGFA). ICU patients with COVID-19 produced higher levels of IL-6 than those not requiring ICU care [44]. According to a meta-analysis, mean IL-6 serum levels are2.9 times higher in patients with severe disease than in those with nonsevere disease [45]. HighIL-6 levels are closely correlated with the serum SARS-CoV-2 viral load, which further affects vital signs and the occurrence of ARDS inCOVID-19 patients [46]. Moreover, as a mediator of SASP, IL-6 is the main functional marker of cell aging [5, 47], and the increase in IL-6 content may correspond to the age-dependent increase in mortality of COVID-19 patients [48]. ...
Detectable serum SARS-CoV-2 viral load (RNAaemia) is closely correlated with drastically elevated interleukin 6 (IL-6) level in critically ill COVID-19 patients
1
2020
... Cytokine storms, namely, hypercytokinemia, a frequent feature of severe SARS, MERS, H5N1 influenza and H7N9 influenza, are associated with disease severity and are a predictor of prognosis [40-42]. Accumulating data suggest that depletion of lymphocytes, activation of cytotoxic T-lymphocytes, neutrophils and neutrophil-mediated cytokine storms may play key roles in COVID-19 pathogenesis [43]. COVID-19 results in increased levels of plasma cytokines, including interleukin-6 (IL-6), interleukin-1β (IL-1β), interleukin-7 (IL-7), interleukin-8 (IL-8), interleukin-9 (IL-9), interleukin-10 (IL-10), granulocyte colony stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), interferon-γ (IFN-γ), tumor necrosis factor (TNF-α) and vascular endothelial growth factor A (VEGFA). ICU patients with COVID-19 produced higher levels of IL-6 than those not requiring ICU care [44]. According to a meta-analysis, mean IL-6 serum levels are2.9 times higher in patients with severe disease than in those with nonsevere disease [45]. HighIL-6 levels are closely correlated with the serum SARS-CoV-2 viral load, which further affects vital signs and the occurrence of ARDS inCOVID-19 patients [46]. Moreover, as a mediator of SASP, IL-6 is the main functional marker of cell aging [5, 47], and the increase in IL-6 content may correspond to the age-dependent increase in mortality of COVID-19 patients [48]. ...
Interleukin-6: a cytokine for gerontologists
1
1993
... Cytokine storms, namely, hypercytokinemia, a frequent feature of severe SARS, MERS, H5N1 influenza and H7N9 influenza, are associated with disease severity and are a predictor of prognosis [40-42]. Accumulating data suggest that depletion of lymphocytes, activation of cytotoxic T-lymphocytes, neutrophils and neutrophil-mediated cytokine storms may play key roles in COVID-19 pathogenesis [43]. COVID-19 results in increased levels of plasma cytokines, including interleukin-6 (IL-6), interleukin-1β (IL-1β), interleukin-7 (IL-7), interleukin-8 (IL-8), interleukin-9 (IL-9), interleukin-10 (IL-10), granulocyte colony stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), interferon-γ (IFN-γ), tumor necrosis factor (TNF-α) and vascular endothelial growth factor A (VEGFA). ICU patients with COVID-19 produced higher levels of IL-6 than those not requiring ICU care [44]. According to a meta-analysis, mean IL-6 serum levels are2.9 times higher in patients with severe disease than in those with nonsevere disease [45]. HighIL-6 levels are closely correlated with the serum SARS-CoV-2 viral load, which further affects vital signs and the occurrence of ARDS inCOVID-19 patients [46]. Moreover, as a mediator of SASP, IL-6 is the main functional marker of cell aging [5, 47], and the increase in IL-6 content may correspond to the age-dependent increase in mortality of COVID-19 patients [48]. ...
COVID-19: A New Virus, but a Familiar Receptor and Cytokine Release Syndrome
1
2020
... Cytokine storms, namely, hypercytokinemia, a frequent feature of severe SARS, MERS, H5N1 influenza and H7N9 influenza, are associated with disease severity and are a predictor of prognosis [40-42]. Accumulating data suggest that depletion of lymphocytes, activation of cytotoxic T-lymphocytes, neutrophils and neutrophil-mediated cytokine storms may play key roles in COVID-19 pathogenesis [43]. COVID-19 results in increased levels of plasma cytokines, including interleukin-6 (IL-6), interleukin-1β (IL-1β), interleukin-7 (IL-7), interleukin-8 (IL-8), interleukin-9 (IL-9), interleukin-10 (IL-10), granulocyte colony stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), interferon-γ (IFN-γ), tumor necrosis factor (TNF-α) and vascular endothelial growth factor A (VEGFA). ICU patients with COVID-19 produced higher levels of IL-6 than those not requiring ICU care [44]. According to a meta-analysis, mean IL-6 serum levels are2.9 times higher in patients with severe disease than in those with nonsevere disease [45]. HighIL-6 levels are closely correlated with the serum SARS-CoV-2 viral load, which further affects vital signs and the occurrence of ARDS inCOVID-19 patients [46]. Moreover, as a mediator of SASP, IL-6 is the main functional marker of cell aging [5, 47], and the increase in IL-6 content may correspond to the age-dependent increase in mortality of COVID-19 patients [48]. ...
SARS and MERS: recent insights into emerging coronaviruses
1
2016
... ACE2 participates in the RAS and plays an important role in regulating IL-6-induced inflammatory injury through the NF-κB and STAT3 pathways [49]. Kubaet al. indicated that SARS-CoV infection could cause a reduction of ACE2 levels on cells, followed by increased serum AngII levels [50]. AngII is one of the key activators of NF-κB and STAT3, which stimulates the expression of IL-6[51]. In turn, we speculate that severe lung inflammation induced by SARS-CoV-2 infection may induce the dysregulation of the RAS followed by the development of ARDS. ...
A crucial role of angiotensin converting enzyme 2 (ACE2) in SARS coronavirus-induced lung injury
1
2005
... ACE2 participates in the RAS and plays an important role in regulating IL-6-induced inflammatory injury through the NF-κB and STAT3 pathways [49]. Kubaet al. indicated that SARS-CoV infection could cause a reduction of ACE2 levels on cells, followed by increased serum AngII levels [50]. AngII is one of the key activators of NF-κB and STAT3, which stimulates the expression of IL-6[51]. In turn, we speculate that severe lung inflammation induced by SARS-CoV-2 infection may induce the dysregulation of the RAS followed by the development of ARDS. ...
Qishenyiqi protects ligation-induced left ventricular remodeling by attenuating inflammation and fibrosis via STAT3 and NF-kappaB signaling pathway
1
2014
... ACE2 participates in the RAS and plays an important role in regulating IL-6-induced inflammatory injury through the NF-κB and STAT3 pathways [49]. Kubaet al. indicated that SARS-CoV infection could cause a reduction of ACE2 levels on cells, followed by increased serum AngII levels [50]. AngII is one of the key activators of NF-κB and STAT3, which stimulates the expression of IL-6[51]. In turn, we speculate that severe lung inflammation induced by SARS-CoV-2 infection may induce the dysregulation of the RAS followed by the development of ARDS. ...
DPP4 inhibition: preventing SARS-CoV-2 infection and/or progression of COVID-19?
1
2020
... CD26, also known as dipeptidyl peptidase 4 (DPP4), is a serine exopeptidase that is expressed ubiquitously in human tissues, including lung, kidney, liver, gut, and immune cell s(including T-cells, activated B-cells, activated natural killer cells and myeloid cells) [52, 53]. CD26 plays multiple roles in nutrition, metabolism, and the immune and endocrine systems. Using mass spectrometry analysis, Kim et al. identified CD26 as a surface protein that is expressed at significantly higher levels in senescent cells. CD26 activity is higher in older than in younger individuals [54]. Overly upregulated CD26 expression and activity are associated with diabetes, obesity and metabolic syndrome, which are reported to influence COVID-19 severity [22, 55]. ...
Genomic organization, exact localization, and tissue expression of the human CD26 (dipeptidyl peptidase IV) gene
1
1994
... CD26, also known as dipeptidyl peptidase 4 (DPP4), is a serine exopeptidase that is expressed ubiquitously in human tissues, including lung, kidney, liver, gut, and immune cell s(including T-cells, activated B-cells, activated natural killer cells and myeloid cells) [52, 53]. CD26 plays multiple roles in nutrition, metabolism, and the immune and endocrine systems. Using mass spectrometry analysis, Kim et al. identified CD26 as a surface protein that is expressed at significantly higher levels in senescent cells. CD26 activity is higher in older than in younger individuals [54]. Overly upregulated CD26 expression and activity are associated with diabetes, obesity and metabolic syndrome, which are reported to influence COVID-19 severity [22, 55]. ...
Identification of senescent cell surface targetable protein DPP4
1
2017
... CD26, also known as dipeptidyl peptidase 4 (DPP4), is a serine exopeptidase that is expressed ubiquitously in human tissues, including lung, kidney, liver, gut, and immune cell s(including T-cells, activated B-cells, activated natural killer cells and myeloid cells) [52, 53]. CD26 plays multiple roles in nutrition, metabolism, and the immune and endocrine systems. Using mass spectrometry analysis, Kim et al. identified CD26 as a surface protein that is expressed at significantly higher levels in senescent cells. CD26 activity is higher in older than in younger individuals [54]. Overly upregulated CD26 expression and activity are associated with diabetes, obesity and metabolic syndrome, which are reported to influence COVID-19 severity [22, 55]. ...
Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases From the Chinese Center for Disease Control and Prevention
1
2020
... CD26, also known as dipeptidyl peptidase 4 (DPP4), is a serine exopeptidase that is expressed ubiquitously in human tissues, including lung, kidney, liver, gut, and immune cell s(including T-cells, activated B-cells, activated natural killer cells and myeloid cells) [52, 53]. CD26 plays multiple roles in nutrition, metabolism, and the immune and endocrine systems. Using mass spectrometry analysis, Kim et al. identified CD26 as a surface protein that is expressed at significantly higher levels in senescent cells. CD26 activity is higher in older than in younger individuals [54]. Overly upregulated CD26 expression and activity are associated with diabetes, obesity and metabolic syndrome, which are reported to influence COVID-19 severity [22, 55]. ...
Middle East Respiratory Syndrome Coronavirus (MERS-CoV): Infection, Immunological Response, and Vaccine Development
1
2019
... Moreover, CD26 has been identified as the functional receptor of MERS-CoV [56, 57]. Research has indicated that MERS-CoV is associated with higher mortality among elderly populations with chronic debilitating diseases including diabetes, malignancy, pulmonary and renal diseases. MERS also appears with greater severity and higher mortality rates in elderly people, especially those with debilitated immune systemsorpre-existing comorbidities [58-60]. Therefore, we suggest that similar to the case for ACE2, DPP4 upregulation may be adeterminant of COVID-19 progression and prognosis. ...
Dipeptidyl peptidase 4 is a functional receptor for the emerging human coronavirus-EMC
1
2013
... Moreover, CD26 has been identified as the functional receptor of MERS-CoV [56, 57]. Research has indicated that MERS-CoV is associated with higher mortality among elderly populations with chronic debilitating diseases including diabetes, malignancy, pulmonary and renal diseases. MERS also appears with greater severity and higher mortality rates in elderly people, especially those with debilitated immune systemsorpre-existing comorbidities [58-60]. Therefore, we suggest that similar to the case for ACE2, DPP4 upregulation may be adeterminant of COVID-19 progression and prognosis. ...
Middle East Respiratory Syndrome Coronavirus (MERS-CoV) infection: epidemiology, pathogenesis and clinical characteristics
1
2018
... Moreover, CD26 has been identified as the functional receptor of MERS-CoV [56, 57]. Research has indicated that MERS-CoV is associated with higher mortality among elderly populations with chronic debilitating diseases including diabetes, malignancy, pulmonary and renal diseases. MERS also appears with greater severity and higher mortality rates in elderly people, especially those with debilitated immune systemsorpre-existing comorbidities [58-60]. Therefore, we suggest that similar to the case for ACE2, DPP4 upregulation may be adeterminant of COVID-19 progression and prognosis. ...
Molecular pathology of emerging coronavirus infections
0
2015
The predictors of 3- and 30-day mortality in 660 MERS-CoV patients
1
2017
... Moreover, CD26 has been identified as the functional receptor of MERS-CoV [56, 57]. Research has indicated that MERS-CoV is associated with higher mortality among elderly populations with chronic debilitating diseases including diabetes, malignancy, pulmonary and renal diseases. MERS also appears with greater severity and higher mortality rates in elderly people, especially those with debilitated immune systemsorpre-existing comorbidities [58-60]. Therefore, we suggest that similar to the case for ACE2, DPP4 upregulation may be adeterminant of COVID-19 progression and prognosis. ...
Cut to the chase: a review of CD26/dipeptidyl peptidase-4's (DPP4) entanglement in the immune system
1
2016
... Large numbers of studies have demonstrated the integral role of CD26 in T lymphocyte activation during immunesenescence and costimulation [61]. CD26 acts as a costimulatory agent that mediates T cell activation by binding to the ligand adenosine deaminase [62]. Additionally, CD26 enhances lymphocyte proliferation independent of ADA [63]. ...
Binding to human dipeptidyl peptidase IV by adenosine deaminase and antibodies that inhibit ligand binding involves overlapping, discontinuous sites on a predicted beta propeller domain
1
1999
... Large numbers of studies have demonstrated the integral role of CD26 in T lymphocyte activation during immunesenescence and costimulation [61]. CD26 acts as a costimulatory agent that mediates T cell activation by binding to the ligand adenosine deaminase [62]. Additionally, CD26 enhances lymphocyte proliferation independent of ADA [63]. ...
Soluble CD26 / dipeptidyl peptidase IV enhances human lymphocyte proliferation in vitro independent of dipeptidyl peptidase enzyme activity and adenosine deaminase binding
1
2011
... Large numbers of studies have demonstrated the integral role of CD26 in T lymphocyte activation during immunesenescence and costimulation [61]. CD26 acts as a costimulatory agent that mediates T cell activation by binding to the ligand adenosine deaminase [62]. Additionally, CD26 enhances lymphocyte proliferation independent of ADA [63]. ...
On the origin of serum CD26 and its altered concentration in cancer patients
1
2009
... CD26 can exist in a soluble form that is considered to be released from the membrane into the plasma, which still retains its enzymatic activity[64]. Ikeda et al. found that soluble CD26 enhances the binding of transcription factors to the TNF-α and IL-6 promoters, thus increasing TNF-α and IL-6 mRNA and protein expression in THP-1 cells [65]. CD26 inhibitors decrease the concentration of proinflammatory factors, such as TNF-α and IL-6 [66]. Thus, some researchers have suggested that the activation of CD26 on T lymphocytes may partially contribute to the high expression of IL-6 in COVID-19 patients. However, the specific role of CD26 in COVID-19 still requires further exploration (Figure 1). ...
Soluble CD26/Dipeptidyl Peptidase IV Enhances the Transcription of IL-6 and TNF-alpha in THP-1 Cells and Monocytes
1
2013
... CD26 can exist in a soluble form that is considered to be released from the membrane into the plasma, which still retains its enzymatic activity[64]. Ikeda et al. found that soluble CD26 enhances the binding of transcription factors to the TNF-α and IL-6 promoters, thus increasing TNF-α and IL-6 mRNA and protein expression in THP-1 cells [65]. CD26 inhibitors decrease the concentration of proinflammatory factors, such as TNF-α and IL-6 [66]. Thus, some researchers have suggested that the activation of CD26 on T lymphocytes may partially contribute to the high expression of IL-6 in COVID-19 patients. However, the specific role of CD26 in COVID-19 still requires further exploration (Figure 1). ...
Neuroprotective Properties of Linagliptin: Focus on Biochemical Mechanisms in Cerebral Ischemia, Vascular Dysfunction and Certain Neurodegenerative Diseases
2
2019
... CD26 can exist in a soluble form that is considered to be released from the membrane into the plasma, which still retains its enzymatic activity[64]. Ikeda et al. found that soluble CD26 enhances the binding of transcription factors to the TNF-α and IL-6 promoters, thus increasing TNF-α and IL-6 mRNA and protein expression in THP-1 cells [65]. CD26 inhibitors decrease the concentration of proinflammatory factors, such as TNF-α and IL-6 [66]. Thus, some researchers have suggested that the activation of CD26 on T lymphocytes may partially contribute to the high expression of IL-6 in COVID-19 patients. However, the specific role of CD26 in COVID-19 still requires further exploration (Figure 1). ...
... The clinical immune response to SARS-CoV-2 can be divided into 2 phases: an earlier phase of elimination by antiviral adaptive immunity and a later phase of damaged alveolar cells triggering innate inflammation [124]. According to Chen et al., the occurrence of ARDS may be associated with the later immune phase, and treatment to reduce inflammation during that phase may help reduce lung damage. CD26 inhibitors may potentially act to regulate an overactive immune reaction and prevent devastating lung injury [125]. In a mouse model of ARDS, which is the main cause of death in COVID-19 patients, CD26 inhibition by sitagliptin alleviated histological findings of lung injury by inhibiting the expression of IL-1β, TNF-α, and IL-6[126]. Birnbaum et al. reported that saxagliptin-mediated DPP4 inhibition could attenuate diabetes mellitus (DM) -induced activation of nod-like receptor family pyrin domain-containing 3 (NLRP3) inflammatory bodies, thus reducing serum CRP, TNF-α, IL-1β, IL-18 and IL-6 levels [127]. CD26 inhibitors, including sitagliptin, alogliptin, vildagliptin, saxagliptin, and linagliptin, are a class of drugs used effectively in the treatment of type 2 diabetes, which has demonstrated safety in elderly patients. These drugs have similar effects by binding to essentially the same catalytic site [128]. Research has shown that the administration of linagliptin can lead to a decrease in the concentration of proinflammatory factors, especially TNF-α and IL-6 [66]. Moreover, mathematical modeling has shown that the spread of MERS-CoV infection can be controlled by inhibiting the expression of CD26, with similar efficiency in SARS-CoV-2 infection [129]. Since the expression of CD26 is closely related to the pathogenesis and severity of COVID-19, CD26 inhibitors have recently been proposed as potential drugsagainst COVID-19 [130]. However, despite laboratory verification and theoretical feasibility, the actual efficacies of CD26 inhibitors in COVID-19 still require verification in further clinical trials. ...
Rapid Progression to Acute Respiratory Distress Syndrome: Review of Current Understanding of Critical Illness from COVID-19 Infection
1
2020
... Current evidence suggests that elderly patients with past comorbidities or dyspnea should be closely monitored for signs of disease progression, decompensation, and exacerbation of illness, especially 1-2 weeks after the onset of symptoms[10, 67]. Presently, there are no officially approved medicines available against SARS-CoV-2. Although the management of COVID-19 patients is primarily supportive, specific therapies are still under investigation. These therapies include current and potential antiviral drugs, anti-senescence drugs, immunosuppressive agents, steroids, mesenchymal stem cell (MSC) transplantation, and an artificial liver system (ALS), among others (Table 1). In the following paragraphs, we aim to highlight the proposed therapeutic strategies [68]. ...
COVID-19: what has been learned and to be learned about the novel coronavirus disease
2
2020
... Current evidence suggests that elderly patients with past comorbidities or dyspnea should be closely monitored for signs of disease progression, decompensation, and exacerbation of illness, especially 1-2 weeks after the onset of symptoms[10, 67]. Presently, there are no officially approved medicines available against SARS-CoV-2. Although the management of COVID-19 patients is primarily supportive, specific therapies are still under investigation. These therapies include current and potential antiviral drugs, anti-senescence drugs, immunosuppressive agents, steroids, mesenchymal stem cell (MSC) transplantation, and an artificial liver system (ALS), among others (Table 1). In the following paragraphs, we aim to highlight the proposed therapeutic strategies [68]. ...
... The development of a safe and effective vaccine against SARS-CoV-2 for nonimmune individuals is an urgent and critical task for controlling the ongoing pandemic [68]. The developing coronavirus vaccines and drugs mainly target the spike glycoprotein or S protein, the major inducers of neutralizing antibodies. To date, Wei Chen et al. conducted a dose-escalation, single-center, open-label, nonrandomized, first-in-human trial of a recombinant adenovirus type5-vectored COVID-19 vaccine in Wuhan, China. The vaccine was tolerable and immunogenic 28 days after vaccination. The humoral responses against SARS-CoV-2 peaked at day 28 after vaccination in healthy adults, and rapid specific T-cell responses were noted from day 14 after vaccination [158]. ...
Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study
1
2020
... Timely antiviral therapy is highly recommended early the course of COVID-19 patients, especially elderly patients and patients with underlying conditions. Wu et al. retrospectively investigated the clinical data of 280 COVID-19 cases and recommended that timely antiviral treatment should be initiated to slow disease progression and improve prognosis in elderly patients [2]. Previously, oseltamivir, which could reduce the mortality of influenza patients, and ganciclovir, which is primarily used to treat cytomegalovirus [69], were widely used for SARS-CoV-2 patients. However, the efficiencies of neuraminidase inhibitors are currently being questioned, which makes them beyond recommendation [70, 71]. ...
A global treatments for coronaviruses including COVID-19
1
2020
... Timely antiviral therapy is highly recommended early the course of COVID-19 patients, especially elderly patients and patients with underlying conditions. Wu et al. retrospectively investigated the clinical data of 280 COVID-19 cases and recommended that timely antiviral treatment should be initiated to slow disease progression and improve prognosis in elderly patients [2]. Previously, oseltamivir, which could reduce the mortality of influenza patients, and ganciclovir, which is primarily used to treat cytomegalovirus [69], were widely used for SARS-CoV-2 patients. However, the efficiencies of neuraminidase inhibitors are currently being questioned, which makes them beyond recommendation [70, 71]. ...
Therapeutic options for the 2019 novel coronavirus (2019-nCoV)
1
2020
... Timely antiviral therapy is highly recommended early the course of COVID-19 patients, especially elderly patients and patients with underlying conditions. Wu et al. retrospectively investigated the clinical data of 280 COVID-19 cases and recommended that timely antiviral treatment should be initiated to slow disease progression and improve prognosis in elderly patients [2]. Previously, oseltamivir, which could reduce the mortality of influenza patients, and ganciclovir, which is primarily used to treat cytomegalovirus [69], were widely used for SARS-CoV-2 patients. However, the efficiencies of neuraminidase inhibitors are currently being questioned, which makes them beyond recommendation [70, 71]. ...
Broad spectrum antiviral remdesivir inhibits human endemic and zoonotic deltacoronaviruses with a highly divergent RNA dependent RNA polymerase
2
2019
... Remdesivir (GS-5734) is a monophosphoramidate prodrug of an adenosine analog that can affect viral RNA polymerase and reduce the production of viral RNA [72]. Remdesivir has shown a significant therapeutic effect in MERS-CoV mouse models [73]. It is effective in the EC50 range of 0.069 μM for SARS-CoV and 0.074 μM for MERS-CoV in tissue cultures as well as 0.77 μM in Vero E6 cells [72, 74]. Theoretically, remdesivir is currently the most promising drug for treating COVID-19. According to the result of a prospective, open-label study of remdesivir, Antinori et al. indicated that this drug could benefit hospitalized patients with SARS-CoV-2 pneumonia, with fewer adverse events observed [75]. The clinical trial conducted by Wang et al. in 237 patients at ten hospitals in Hubei Province showed that, although not statistically significant, the patients receiving remdesivir had a faster time to clinical improvement than those receiving placebo [76]. In the trial conducted by Beigel and colleagues, 1063 COVID-19 patients were randomly assigned to remdesivir or placebo. The results showed that remdesivir could obviously shorten the recovery time in hospitalized COVID-19 patients [77]. The authors also emphasized that earlier remdesivir treatment was probably more beneficial than later treatment [78]. Further explorations of the safety and efficiency of remdesivir for COVID-19 are still ongoing. ...
... ]. It is effective in the EC50 range of 0.069 μM for SARS-CoV and 0.074 μM for MERS-CoV in tissue cultures as well as 0.77 μM in Vero E6 cells [72, 74]. Theoretically, remdesivir is currently the most promising drug for treating COVID-19. According to the result of a prospective, open-label study of remdesivir, Antinori et al. indicated that this drug could benefit hospitalized patients with SARS-CoV-2 pneumonia, with fewer adverse events observed [75]. The clinical trial conducted by Wang et al. in 237 patients at ten hospitals in Hubei Province showed that, although not statistically significant, the patients receiving remdesivir had a faster time to clinical improvement than those receiving placebo [76]. In the trial conducted by Beigel and colleagues, 1063 COVID-19 patients were randomly assigned to remdesivir or placebo. The results showed that remdesivir could obviously shorten the recovery time in hospitalized COVID-19 patients [77]. The authors also emphasized that earlier remdesivir treatment was probably more beneficial than later treatment [78]. Further explorations of the safety and efficiency of remdesivir for COVID-19 are still ongoing. ...
Comparative therapeutic efficacy of remdesivir and combination lopinavir, ritonavir, and interferon beta against MERS-CoV
1
2020
... Remdesivir (GS-5734) is a monophosphoramidate prodrug of an adenosine analog that can affect viral RNA polymerase and reduce the production of viral RNA [72]. Remdesivir has shown a significant therapeutic effect in MERS-CoV mouse models [73]. It is effective in the EC50 range of 0.069 μM for SARS-CoV and 0.074 μM for MERS-CoV in tissue cultures as well as 0.77 μM in Vero E6 cells [72, 74]. Theoretically, remdesivir is currently the most promising drug for treating COVID-19. According to the result of a prospective, open-label study of remdesivir, Antinori et al. indicated that this drug could benefit hospitalized patients with SARS-CoV-2 pneumonia, with fewer adverse events observed [75]. The clinical trial conducted by Wang et al. in 237 patients at ten hospitals in Hubei Province showed that, although not statistically significant, the patients receiving remdesivir had a faster time to clinical improvement than those receiving placebo [76]. In the trial conducted by Beigel and colleagues, 1063 COVID-19 patients were randomly assigned to remdesivir or placebo. The results showed that remdesivir could obviously shorten the recovery time in hospitalized COVID-19 patients [77]. The authors also emphasized that earlier remdesivir treatment was probably more beneficial than later treatment [78]. Further explorations of the safety and efficiency of remdesivir for COVID-19 are still ongoing. ...
A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe Covid-19
2
2020
... Remdesivir (GS-5734) is a monophosphoramidate prodrug of an adenosine analog that can affect viral RNA polymerase and reduce the production of viral RNA [72]. Remdesivir has shown a significant therapeutic effect in MERS-CoV mouse models [73]. It is effective in the EC50 range of 0.069 μM for SARS-CoV and 0.074 μM for MERS-CoV in tissue cultures as well as 0.77 μM in Vero E6 cells [72, 74]. Theoretically, remdesivir is currently the most promising drug for treating COVID-19. According to the result of a prospective, open-label study of remdesivir, Antinori et al. indicated that this drug could benefit hospitalized patients with SARS-CoV-2 pneumonia, with fewer adverse events observed [75]. The clinical trial conducted by Wang et al. in 237 patients at ten hospitals in Hubei Province showed that, although not statistically significant, the patients receiving remdesivir had a faster time to clinical improvement than those receiving placebo [76]. In the trial conducted by Beigel and colleagues, 1063 COVID-19 patients were randomly assigned to remdesivir or placebo. The results showed that remdesivir could obviously shorten the recovery time in hospitalized COVID-19 patients [77]. The authors also emphasized that earlier remdesivir treatment was probably more beneficial than later treatment [78]. Further explorations of the safety and efficiency of remdesivir for COVID-19 are still ongoing. ...
... Lopinavir/ritonavir (LPV/RTV),which acts as antiretroviral protease inhibitor, is used as an anti-HIV drug [79]. In India, the Central Drugs Standard Control Organization approved the restricted public health use of the LPV/RTV combination in symptomatic COVID-19 patients [80]. However, the efficacy of LPV/RTV for COVID-19 is still controversial. A clinical trial in Hubei showed that early LPV/RTV treatment could shorten the viral shedding duration in COVID-19 patients, especially in those of an older age [81]. Cheng et al. obtained the exact opposite result among patients with mild pneumonia in Taiwan [82]. According to a randomized, controlled, open-label trial in 199 patients with severe COVID-19, mortality at 28 days and viral clearance time were similar in the LPV/RTV group and the standard-care group. The results suggested that no benefit was observed with LPV/RTV treatment [74]. Therefore, the WHO suggested larger trials with a greater variety of COVID-19 patients [83]. ...
Compassionate remdesivir treatment of severe Covid-19 pneumonia in intensive care unit (ICU) and Non-ICU patients: Clinical outcome and differences in post-treatment hospitalisation status
1
2020
... Remdesivir (GS-5734) is a monophosphoramidate prodrug of an adenosine analog that can affect viral RNA polymerase and reduce the production of viral RNA [72]. Remdesivir has shown a significant therapeutic effect in MERS-CoV mouse models [73]. It is effective in the EC50 range of 0.069 μM for SARS-CoV and 0.074 μM for MERS-CoV in tissue cultures as well as 0.77 μM in Vero E6 cells [72, 74]. Theoretically, remdesivir is currently the most promising drug for treating COVID-19. According to the result of a prospective, open-label study of remdesivir, Antinori et al. indicated that this drug could benefit hospitalized patients with SARS-CoV-2 pneumonia, with fewer adverse events observed [75]. The clinical trial conducted by Wang et al. in 237 patients at ten hospitals in Hubei Province showed that, although not statistically significant, the patients receiving remdesivir had a faster time to clinical improvement than those receiving placebo [76]. In the trial conducted by Beigel and colleagues, 1063 COVID-19 patients were randomly assigned to remdesivir or placebo. The results showed that remdesivir could obviously shorten the recovery time in hospitalized COVID-19 patients [77]. The authors also emphasized that earlier remdesivir treatment was probably more beneficial than later treatment [78]. Further explorations of the safety and efficiency of remdesivir for COVID-19 are still ongoing. ...
Remdesivir in adults with severe COVID-19: a randomised, double-blind, placebo-controlled, multicentre trial
1
2020
... Remdesivir (GS-5734) is a monophosphoramidate prodrug of an adenosine analog that can affect viral RNA polymerase and reduce the production of viral RNA [72]. Remdesivir has shown a significant therapeutic effect in MERS-CoV mouse models [73]. It is effective in the EC50 range of 0.069 μM for SARS-CoV and 0.074 μM for MERS-CoV in tissue cultures as well as 0.77 μM in Vero E6 cells [72, 74]. Theoretically, remdesivir is currently the most promising drug for treating COVID-19. According to the result of a prospective, open-label study of remdesivir, Antinori et al. indicated that this drug could benefit hospitalized patients with SARS-CoV-2 pneumonia, with fewer adverse events observed [75]. The clinical trial conducted by Wang et al. in 237 patients at ten hospitals in Hubei Province showed that, although not statistically significant, the patients receiving remdesivir had a faster time to clinical improvement than those receiving placebo [76]. In the trial conducted by Beigel and colleagues, 1063 COVID-19 patients were randomly assigned to remdesivir or placebo. The results showed that remdesivir could obviously shorten the recovery time in hospitalized COVID-19 patients [77]. The authors also emphasized that earlier remdesivir treatment was probably more beneficial than later treatment [78]. Further explorations of the safety and efficiency of remdesivir for COVID-19 are still ongoing. ...
Remdesivir for the Treatment of Covid-19 - Preliminary Report
1
2020
... Remdesivir (GS-5734) is a monophosphoramidate prodrug of an adenosine analog that can affect viral RNA polymerase and reduce the production of viral RNA [72]. Remdesivir has shown a significant therapeutic effect in MERS-CoV mouse models [73]. It is effective in the EC50 range of 0.069 μM for SARS-CoV and 0.074 μM for MERS-CoV in tissue cultures as well as 0.77 μM in Vero E6 cells [72, 74]. Theoretically, remdesivir is currently the most promising drug for treating COVID-19. According to the result of a prospective, open-label study of remdesivir, Antinori et al. indicated that this drug could benefit hospitalized patients with SARS-CoV-2 pneumonia, with fewer adverse events observed [75]. The clinical trial conducted by Wang et al. in 237 patients at ten hospitals in Hubei Province showed that, although not statistically significant, the patients receiving remdesivir had a faster time to clinical improvement than those receiving placebo [76]. In the trial conducted by Beigel and colleagues, 1063 COVID-19 patients were randomly assigned to remdesivir or placebo. The results showed that remdesivir could obviously shorten the recovery time in hospitalized COVID-19 patients [77]. The authors also emphasized that earlier remdesivir treatment was probably more beneficial than later treatment [78]. Further explorations of the safety and efficiency of remdesivir for COVID-19 are still ongoing. ...
Remdesivir for the Treatment of Covid-19 - Preliminary Report
1
2020
... Remdesivir (GS-5734) is a monophosphoramidate prodrug of an adenosine analog that can affect viral RNA polymerase and reduce the production of viral RNA [72]. Remdesivir has shown a significant therapeutic effect in MERS-CoV mouse models [73]. It is effective in the EC50 range of 0.069 μM for SARS-CoV and 0.074 μM for MERS-CoV in tissue cultures as well as 0.77 μM in Vero E6 cells [72, 74]. Theoretically, remdesivir is currently the most promising drug for treating COVID-19. According to the result of a prospective, open-label study of remdesivir, Antinori et al. indicated that this drug could benefit hospitalized patients with SARS-CoV-2 pneumonia, with fewer adverse events observed [75]. The clinical trial conducted by Wang et al. in 237 patients at ten hospitals in Hubei Province showed that, although not statistically significant, the patients receiving remdesivir had a faster time to clinical improvement than those receiving placebo [76]. In the trial conducted by Beigel and colleagues, 1063 COVID-19 patients were randomly assigned to remdesivir or placebo. The results showed that remdesivir could obviously shorten the recovery time in hospitalized COVID-19 patients [77]. The authors also emphasized that earlier remdesivir treatment was probably more beneficial than later treatment [78]. Further explorations of the safety and efficiency of remdesivir for COVID-19 are still ongoing. ...
Literature-based review of the drugs used for the treatment of COVID-19
1
2020
... Lopinavir/ritonavir (LPV/RTV),which acts as antiretroviral protease inhibitor, is used as an anti-HIV drug [79]. In India, the Central Drugs Standard Control Organization approved the restricted public health use of the LPV/RTV combination in symptomatic COVID-19 patients [80]. However, the efficacy of LPV/RTV for COVID-19 is still controversial. A clinical trial in Hubei showed that early LPV/RTV treatment could shorten the viral shedding duration in COVID-19 patients, especially in those of an older age [81]. Cheng et al. obtained the exact opposite result among patients with mild pneumonia in Taiwan [82]. According to a randomized, controlled, open-label trial in 199 patients with severe COVID-19, mortality at 28 days and viral clearance time were similar in the LPV/RTV group and the standard-care group. The results suggested that no benefit was observed with LPV/RTV treatment [74]. Therefore, the WHO suggested larger trials with a greater variety of COVID-19 patients [83]. ...
Lopinavir/ritonavir combination therapy amongst symptomatic coronavirus disease 2019 patients in India: Protocol for restricted public health emergency use
1
2020
... Lopinavir/ritonavir (LPV/RTV),which acts as antiretroviral protease inhibitor, is used as an anti-HIV drug [79]. In India, the Central Drugs Standard Control Organization approved the restricted public health use of the LPV/RTV combination in symptomatic COVID-19 patients [80]. However, the efficacy of LPV/RTV for COVID-19 is still controversial. A clinical trial in Hubei showed that early LPV/RTV treatment could shorten the viral shedding duration in COVID-19 patients, especially in those of an older age [81]. Cheng et al. obtained the exact opposite result among patients with mild pneumonia in Taiwan [82]. According to a randomized, controlled, open-label trial in 199 patients with severe COVID-19, mortality at 28 days and viral clearance time were similar in the LPV/RTV group and the standard-care group. The results suggested that no benefit was observed with LPV/RTV treatment [74]. Therefore, the WHO suggested larger trials with a greater variety of COVID-19 patients [83]. ...
Factors associated with prolonged viral shedding and impact of Lopinavir/Ritonavir treatment in hospitalised non-critically ill patients with SARS-CoV-2 infection
1
2020
... Lopinavir/ritonavir (LPV/RTV),which acts as antiretroviral protease inhibitor, is used as an anti-HIV drug [79]. In India, the Central Drugs Standard Control Organization approved the restricted public health use of the LPV/RTV combination in symptomatic COVID-19 patients [80]. However, the efficacy of LPV/RTV for COVID-19 is still controversial. A clinical trial in Hubei showed that early LPV/RTV treatment could shorten the viral shedding duration in COVID-19 patients, especially in those of an older age [81]. Cheng et al. obtained the exact opposite result among patients with mild pneumonia in Taiwan [82]. According to a randomized, controlled, open-label trial in 199 patients with severe COVID-19, mortality at 28 days and viral clearance time were similar in the LPV/RTV group and the standard-care group. The results suggested that no benefit was observed with LPV/RTV treatment [74]. Therefore, the WHO suggested larger trials with a greater variety of COVID-19 patients [83]. ...
Lopinavir/ritonavir did not shorten the duration of SARS CoV-2 shedding in patients with mild pneumonia in Taiwan
1
2020
... Lopinavir/ritonavir (LPV/RTV),which acts as antiretroviral protease inhibitor, is used as an anti-HIV drug [79]. In India, the Central Drugs Standard Control Organization approved the restricted public health use of the LPV/RTV combination in symptomatic COVID-19 patients [80]. However, the efficacy of LPV/RTV for COVID-19 is still controversial. A clinical trial in Hubei showed that early LPV/RTV treatment could shorten the viral shedding duration in COVID-19 patients, especially in those of an older age [81]. Cheng et al. obtained the exact opposite result among patients with mild pneumonia in Taiwan [82]. According to a randomized, controlled, open-label trial in 199 patients with severe COVID-19, mortality at 28 days and viral clearance time were similar in the LPV/RTV group and the standard-care group. The results suggested that no benefit was observed with LPV/RTV treatment [74]. Therefore, the WHO suggested larger trials with a greater variety of COVID-19 patients [83]. ...
SARS-CoV-2: Recent Reports on Antiviral Therapies Based on Lopinavir/Ritonavir, Darunavir/Umifenovir, Hydroxychloroquine, Remdesivir, Favipiravir and Other Drugs for the Treatment of the New Coronavirus
1
2020
... Lopinavir/ritonavir (LPV/RTV),which acts as antiretroviral protease inhibitor, is used as an anti-HIV drug [79]. In India, the Central Drugs Standard Control Organization approved the restricted public health use of the LPV/RTV combination in symptomatic COVID-19 patients [80]. However, the efficacy of LPV/RTV for COVID-19 is still controversial. A clinical trial in Hubei showed that early LPV/RTV treatment could shorten the viral shedding duration in COVID-19 patients, especially in those of an older age [81]. Cheng et al. obtained the exact opposite result among patients with mild pneumonia in Taiwan [82]. According to a randomized, controlled, open-label trial in 199 patients with severe COVID-19, mortality at 28 days and viral clearance time were similar in the LPV/RTV group and the standard-care group. The results suggested that no benefit was observed with LPV/RTV treatment [74]. Therefore, the WHO suggested larger trials with a greater variety of COVID-19 patients [83]. ...
Favipiravir: Pharmacokinetics and Concerns About Clinical Trials for 2019-nCoV Infection
1
2020
... Favipiravir (FPV), a purine nucleic acid analog that targets RNA-dependent RNA polymerase (RdRP), is widely used as an oral anti-influenza drug [84]. Cai et al. conducted a clinical trial to evaluate the safety and efficacy of favipiravir in COVID-19 patients. A shorter viral clearance time as well as a significantly higher improvement rate in chest imaging was shown for the FPV group versus the LPV/r group. In addition, fewer adverse reactions were found in the FPV group than in the LPV/r group [85]. ...
Experimental Treatment with Favipiravir for COVID-19: An Open-Label Control Study
1
2020
... Favipiravir (FPV), a purine nucleic acid analog that targets RNA-dependent RNA polymerase (RdRP), is widely used as an oral anti-influenza drug [84]. Cai et al. conducted a clinical trial to evaluate the safety and efficacy of favipiravir in COVID-19 patients. A shorter viral clearance time as well as a significantly higher improvement rate in chest imaging was shown for the FPV group versus the LPV/r group. In addition, fewer adverse reactions were found in the FPV group than in the LPV/r group [85]. ...
The Location of the Protonated and Unprotonated Forms of Arbidol in the Membrane: A Molecular Dynamics Study
1
2016
... Arbidol, an important anti-viral drug candidate, also showed promising effects in COVID-19. Arbidol is a broad-spectrum antiviral molecule that inhibits both DNA as well as RNA viruses by altering the membrane structure of the virus [86]. According to Zhu et al., patients treated with arbidol show a shorter duration of positive RNA test compared to those treated with LPV/RTV, while nosignificant adverse effects are observed. The results indicated that arbidol monotherapy is superior to LPV/RTVin COVID-19 treatment [87]. Additionally, a retrospective cohort study showed that arbidol combined with LPV/RTV showed improved efficacy in COVID-19 patients [88]. Another retrospective, single-center study showed that the combination of Lianhuaqingwen and arbidol was effective for patients with mild symptoms within 5-7 days, and the cure rate was 98% [89]. Moreover, arbidol is considered to have a preventive effect. Yang et al. suggested that prophylactic oral arbidol was associated with a lower incidence of SARS-CoV-2 infection in medical staff [90]. Although accumulating evidence has demonstrated the potential clinical efficiency of arbidol, powered randomized control trials are still needed for further confirmation [91]. ...
Arbidol monotherapy is superior to lopinavir/ritonavir in treating COVID-19
1
2020
... Arbidol, an important anti-viral drug candidate, also showed promising effects in COVID-19. Arbidol is a broad-spectrum antiviral molecule that inhibits both DNA as well as RNA viruses by altering the membrane structure of the virus [86]. According to Zhu et al., patients treated with arbidol show a shorter duration of positive RNA test compared to those treated with LPV/RTV, while nosignificant adverse effects are observed. The results indicated that arbidol monotherapy is superior to LPV/RTVin COVID-19 treatment [87]. Additionally, a retrospective cohort study showed that arbidol combined with LPV/RTV showed improved efficacy in COVID-19 patients [88]. Another retrospective, single-center study showed that the combination of Lianhuaqingwen and arbidol was effective for patients with mild symptoms within 5-7 days, and the cure rate was 98% [89]. Moreover, arbidol is considered to have a preventive effect. Yang et al. suggested that prophylactic oral arbidol was associated with a lower incidence of SARS-CoV-2 infection in medical staff [90]. Although accumulating evidence has demonstrated the potential clinical efficiency of arbidol, powered randomized control trials are still needed for further confirmation [91]. ...
Arbidol combined with LPV/r versus LPV/r alone against Corona Virus Disease 2019: A retrospective cohort study
1
2020
... Arbidol, an important anti-viral drug candidate, also showed promising effects in COVID-19. Arbidol is a broad-spectrum antiviral molecule that inhibits both DNA as well as RNA viruses by altering the membrane structure of the virus [86]. According to Zhu et al., patients treated with arbidol show a shorter duration of positive RNA test compared to those treated with LPV/RTV, while nosignificant adverse effects are observed. The results indicated that arbidol monotherapy is superior to LPV/RTVin COVID-19 treatment [87]. Additionally, a retrospective cohort study showed that arbidol combined with LPV/RTV showed improved efficacy in COVID-19 patients [88]. Another retrospective, single-center study showed that the combination of Lianhuaqingwen and arbidol was effective for patients with mild symptoms within 5-7 days, and the cure rate was 98% [89]. Moreover, arbidol is considered to have a preventive effect. Yang et al. suggested that prophylactic oral arbidol was associated with a lower incidence of SARS-CoV-2 infection in medical staff [90]. Although accumulating evidence has demonstrated the potential clinical efficiency of arbidol, powered randomized control trials are still needed for further confirmation [91]. ...
COVID-19: Clinical aspects and therapeutics responses
1
2020
... Arbidol, an important anti-viral drug candidate, also showed promising effects in COVID-19. Arbidol is a broad-spectrum antiviral molecule that inhibits both DNA as well as RNA viruses by altering the membrane structure of the virus [86]. According to Zhu et al., patients treated with arbidol show a shorter duration of positive RNA test compared to those treated with LPV/RTV, while nosignificant adverse effects are observed. The results indicated that arbidol monotherapy is superior to LPV/RTVin COVID-19 treatment [87]. Additionally, a retrospective cohort study showed that arbidol combined with LPV/RTV showed improved efficacy in COVID-19 patients [88]. Another retrospective, single-center study showed that the combination of Lianhuaqingwen and arbidol was effective for patients with mild symptoms within 5-7 days, and the cure rate was 98% [89]. Moreover, arbidol is considered to have a preventive effect. Yang et al. suggested that prophylactic oral arbidol was associated with a lower incidence of SARS-CoV-2 infection in medical staff [90]. Although accumulating evidence has demonstrated the potential clinical efficiency of arbidol, powered randomized control trials are still needed for further confirmation [91]. ...
Effectiveness of Arbidol for COVID-19 Prevention in Health Professionals
1
2020
... Arbidol, an important anti-viral drug candidate, also showed promising effects in COVID-19. Arbidol is a broad-spectrum antiviral molecule that inhibits both DNA as well as RNA viruses by altering the membrane structure of the virus [86]. According to Zhu et al., patients treated with arbidol show a shorter duration of positive RNA test compared to those treated with LPV/RTV, while nosignificant adverse effects are observed. The results indicated that arbidol monotherapy is superior to LPV/RTVin COVID-19 treatment [87]. Additionally, a retrospective cohort study showed that arbidol combined with LPV/RTV showed improved efficacy in COVID-19 patients [88]. Another retrospective, single-center study showed that the combination of Lianhuaqingwen and arbidol was effective for patients with mild symptoms within 5-7 days, and the cure rate was 98% [89]. Moreover, arbidol is considered to have a preventive effect. Yang et al. suggested that prophylactic oral arbidol was associated with a lower incidence of SARS-CoV-2 infection in medical staff [90]. Although accumulating evidence has demonstrated the potential clinical efficiency of arbidol, powered randomized control trials are still needed for further confirmation [91]. ...
Clinical efficacy of antivirals against novel coronavirus (COVID-19): A review
1
2020
... Arbidol, an important anti-viral drug candidate, also showed promising effects in COVID-19. Arbidol is a broad-spectrum antiviral molecule that inhibits both DNA as well as RNA viruses by altering the membrane structure of the virus [86]. According to Zhu et al., patients treated with arbidol show a shorter duration of positive RNA test compared to those treated with LPV/RTV, while nosignificant adverse effects are observed. The results indicated that arbidol monotherapy is superior to LPV/RTVin COVID-19 treatment [87]. Additionally, a retrospective cohort study showed that arbidol combined with LPV/RTV showed improved efficacy in COVID-19 patients [88]. Another retrospective, single-center study showed that the combination of Lianhuaqingwen and arbidol was effective for patients with mild symptoms within 5-7 days, and the cure rate was 98% [89]. Moreover, arbidol is considered to have a preventive effect. Yang et al. suggested that prophylactic oral arbidol was associated with a lower incidence of SARS-CoV-2 infection in medical staff [90]. Although accumulating evidence has demonstrated the potential clinical efficiency of arbidol, powered randomized control trials are still needed for further confirmation [91]. ...
Azithromycin and Roxithromycin define a new family of "senolytic" drugs that target senescent human fibroblasts
1
2018
... Azithromycin and the closely related drug roxithromycin are macrolide antibiotics that can act as senolytic drugs that target and remove senescent cells [92]. Additionally, azithromycin is known to exert an antifibrotic effect by significantly extending the lifespan of myofibroblast cells. Moreover, azithromycin has been proven to reduce airway inflammation by inhibiting IL-6 and IL-1β expression in mouse models [93, 94]. Therefore, azithromycin is recommended by a number of researchers as a potential COVID-19 treatment strategy. However, Gbinigie et al. conducted a rapid review of the current literature. The results indicated that other than in the case of bacterial super infection, there was no evidence supporting the use of azithromycin for the treatment of SARS-CoV-2 infection outside of the context of clinical trials [95]. According to a clinical trial conducted by Rosenberg et al., receipt of azithromycin alone could not significantly reduce in-hospital mortality of COVID-19 patients [96]. ...
Role of prophylactic azithromycin to reduce airway inflammation and mortality in a RSV mouse infection model
1
2018
... Azithromycin and the closely related drug roxithromycin are macrolide antibiotics that can act as senolytic drugs that target and remove senescent cells [92]. Additionally, azithromycin is known to exert an antifibrotic effect by significantly extending the lifespan of myofibroblast cells. Moreover, azithromycin has been proven to reduce airway inflammation by inhibiting IL-6 and IL-1β expression in mouse models [93, 94]. Therefore, azithromycin is recommended by a number of researchers as a potential COVID-19 treatment strategy. However, Gbinigie et al. conducted a rapid review of the current literature. The results indicated that other than in the case of bacterial super infection, there was no evidence supporting the use of azithromycin for the treatment of SARS-CoV-2 infection outside of the context of clinical trials [95]. According to a clinical trial conducted by Rosenberg et al., receipt of azithromycin alone could not significantly reduce in-hospital mortality of COVID-19 patients [96]. ...
Azithromycin attenuates acute radiation-induced lung injury in mice
1
2017
... Azithromycin and the closely related drug roxithromycin are macrolide antibiotics that can act as senolytic drugs that target and remove senescent cells [92]. Additionally, azithromycin is known to exert an antifibrotic effect by significantly extending the lifespan of myofibroblast cells. Moreover, azithromycin has been proven to reduce airway inflammation by inhibiting IL-6 and IL-1β expression in mouse models [93, 94]. Therefore, azithromycin is recommended by a number of researchers as a potential COVID-19 treatment strategy. However, Gbinigie et al. conducted a rapid review of the current literature. The results indicated that other than in the case of bacterial super infection, there was no evidence supporting the use of azithromycin for the treatment of SARS-CoV-2 infection outside of the context of clinical trials [95]. According to a clinical trial conducted by Rosenberg et al., receipt of azithromycin alone could not significantly reduce in-hospital mortality of COVID-19 patients [96]. ...
Should azithromycin be used to treat COVID-19? A rapid review
1
2020
... Azithromycin and the closely related drug roxithromycin are macrolide antibiotics that can act as senolytic drugs that target and remove senescent cells [92]. Additionally, azithromycin is known to exert an antifibrotic effect by significantly extending the lifespan of myofibroblast cells. Moreover, azithromycin has been proven to reduce airway inflammation by inhibiting IL-6 and IL-1β expression in mouse models [93, 94]. Therefore, azithromycin is recommended by a number of researchers as a potential COVID-19 treatment strategy. However, Gbinigie et al. conducted a rapid review of the current literature. The results indicated that other than in the case of bacterial super infection, there was no evidence supporting the use of azithromycin for the treatment of SARS-CoV-2 infection outside of the context of clinical trials [95]. According to a clinical trial conducted by Rosenberg et al., receipt of azithromycin alone could not significantly reduce in-hospital mortality of COVID-19 patients [96]. ...
Association of Treatment With Hydroxychloroquine or Azithromycin With In-Hospital Mortality in Patients With COVID-19 in New York State
2
2020
... Azithromycin and the closely related drug roxithromycin are macrolide antibiotics that can act as senolytic drugs that target and remove senescent cells [92]. Additionally, azithromycin is known to exert an antifibrotic effect by significantly extending the lifespan of myofibroblast cells. Moreover, azithromycin has been proven to reduce airway inflammation by inhibiting IL-6 and IL-1β expression in mouse models [93, 94]. Therefore, azithromycin is recommended by a number of researchers as a potential COVID-19 treatment strategy. However, Gbinigie et al. conducted a rapid review of the current literature. The results indicated that other than in the case of bacterial super infection, there was no evidence supporting the use of azithromycin for the treatment of SARS-CoV-2 infection outside of the context of clinical trials [95]. According to a clinical trial conducted by Rosenberg et al., receipt of azithromycin alone could not significantly reduce in-hospital mortality of COVID-19 patients [96]. ...
... Chloroquine (CQ) and its derivative hydroxychloroquine (HCQ) have the ability to induce alkalization, which functionally prevents the induction and accumulation of beta-galactosidase (β-Gal), known as a marker of senescence [97]. CQ and HCQ are widely used antimalarial and antiviral drugs and have recently received much attention as potential treatments for COVID-19 [98].CQ was recently demonstrated as an inhibitor ofSARS-CoV-2 in vitro, and the hydroxylated form, HCQ, has been proven to limit the replication of SARS-CoV-2 in vitro [99, 100]. Huang et al. found that CQ had a slight advantage over lopinavir/ritonavir in COVID-19 patients [101]. HCQ can also specifically inhibit the replication of SARS-CoV by interfering with the glycosylation of ACE2 [102]. Therefore, HCQ has been widely suggested as a potential treatment for patients with SARS-CoV-2 infection. A number of clinical trials have been conducted to explore the efficacies of CQ and HCQ. According to a small open-label nonrandomized clinical trial, HCQ treatment was significantly associated with viral load reduction in COVID-19 patients, and its efficacy could be reinforced by azithromycin [103]. However, according to a newly published comparative observational study among 181 COVID-19 patients with documented severe acute respiratory syndrome who required oxygen, HCQ did not show an obvious therapeutic effect. Additionally, eight patients in the HCQ group (10%) experienced electrocardiographic modifications that required discontinuation of treatment [104]. Despite the controversial results of these clinical trials, frequent side effects of CQ and HCQ, for example, worsening vision, nausea, digestive disorders and potential heart failure and even death, have hindered the wide application of these drugs [105]. Moreover, the results of a clinical trial conducted by Rosenberg et al., which involved 1438 COVID-19 patients, showed that compared with neither treatment, treatment with HCQ alone or combined with azithromycin was not significantly associated with differences in mortality [96]. ...
Senescence-associated (beta)-galactosidase reflects an increase in lysosomal mass during replicative ageing of human endothelial cells
1
2000
... Chloroquine (CQ) and its derivative hydroxychloroquine (HCQ) have the ability to induce alkalization, which functionally prevents the induction and accumulation of beta-galactosidase (β-Gal), known as a marker of senescence [97]. CQ and HCQ are widely used antimalarial and antiviral drugs and have recently received much attention as potential treatments for COVID-19 [98].CQ was recently demonstrated as an inhibitor ofSARS-CoV-2 in vitro, and the hydroxylated form, HCQ, has been proven to limit the replication of SARS-CoV-2 in vitro [99, 100]. Huang et al. found that CQ had a slight advantage over lopinavir/ritonavir in COVID-19 patients [101]. HCQ can also specifically inhibit the replication of SARS-CoV by interfering with the glycosylation of ACE2 [102]. Therefore, HCQ has been widely suggested as a potential treatment for patients with SARS-CoV-2 infection. A number of clinical trials have been conducted to explore the efficacies of CQ and HCQ. According to a small open-label nonrandomized clinical trial, HCQ treatment was significantly associated with viral load reduction in COVID-19 patients, and its efficacy could be reinforced by azithromycin [103]. However, according to a newly published comparative observational study among 181 COVID-19 patients with documented severe acute respiratory syndrome who required oxygen, HCQ did not show an obvious therapeutic effect. Additionally, eight patients in the HCQ group (10%) experienced electrocardiographic modifications that required discontinuation of treatment [104]. Despite the controversial results of these clinical trials, frequent side effects of CQ and HCQ, for example, worsening vision, nausea, digestive disorders and potential heart failure and even death, have hindered the wide application of these drugs [105]. Moreover, the results of a clinical trial conducted by Rosenberg et al., which involved 1438 COVID-19 patients, showed that compared with neither treatment, treatment with HCQ alone or combined with azithromycin was not significantly associated with differences in mortality [96]. ...
Angiotensin-converting enzyme-2 (ACE2), SARS-CoV-2 and pathophysiology of coronavirus disease 2019 (COVID-19)
1
2020
... Chloroquine (CQ) and its derivative hydroxychloroquine (HCQ) have the ability to induce alkalization, which functionally prevents the induction and accumulation of beta-galactosidase (β-Gal), known as a marker of senescence [97]. CQ and HCQ are widely used antimalarial and antiviral drugs and have recently received much attention as potential treatments for COVID-19 [98].CQ was recently demonstrated as an inhibitor ofSARS-CoV-2 in vitro, and the hydroxylated form, HCQ, has been proven to limit the replication of SARS-CoV-2 in vitro [99, 100]. Huang et al. found that CQ had a slight advantage over lopinavir/ritonavir in COVID-19 patients [101]. HCQ can also specifically inhibit the replication of SARS-CoV by interfering with the glycosylation of ACE2 [102]. Therefore, HCQ has been widely suggested as a potential treatment for patients with SARS-CoV-2 infection. A number of clinical trials have been conducted to explore the efficacies of CQ and HCQ. According to a small open-label nonrandomized clinical trial, HCQ treatment was significantly associated with viral load reduction in COVID-19 patients, and its efficacy could be reinforced by azithromycin [103]. However, according to a newly published comparative observational study among 181 COVID-19 patients with documented severe acute respiratory syndrome who required oxygen, HCQ did not show an obvious therapeutic effect. Additionally, eight patients in the HCQ group (10%) experienced electrocardiographic modifications that required discontinuation of treatment [104]. Despite the controversial results of these clinical trials, frequent side effects of CQ and HCQ, for example, worsening vision, nausea, digestive disorders and potential heart failure and even death, have hindered the wide application of these drugs [105]. Moreover, the results of a clinical trial conducted by Rosenberg et al., which involved 1438 COVID-19 patients, showed that compared with neither treatment, treatment with HCQ alone or combined with azithromycin was not significantly associated with differences in mortality [96]. ...
New insights on the antiviral effects of chloroquine against coronavirus: what to expect for COVID-19?
1
2020
... Chloroquine (CQ) and its derivative hydroxychloroquine (HCQ) have the ability to induce alkalization, which functionally prevents the induction and accumulation of beta-galactosidase (β-Gal), known as a marker of senescence [97]. CQ and HCQ are widely used antimalarial and antiviral drugs and have recently received much attention as potential treatments for COVID-19 [98].CQ was recently demonstrated as an inhibitor ofSARS-CoV-2 in vitro, and the hydroxylated form, HCQ, has been proven to limit the replication of SARS-CoV-2 in vitro [99, 100]. Huang et al. found that CQ had a slight advantage over lopinavir/ritonavir in COVID-19 patients [101]. HCQ can also specifically inhibit the replication of SARS-CoV by interfering with the glycosylation of ACE2 [102]. Therefore, HCQ has been widely suggested as a potential treatment for patients with SARS-CoV-2 infection. A number of clinical trials have been conducted to explore the efficacies of CQ and HCQ. According to a small open-label nonrandomized clinical trial, HCQ treatment was significantly associated with viral load reduction in COVID-19 patients, and its efficacy could be reinforced by azithromycin [103]. However, according to a newly published comparative observational study among 181 COVID-19 patients with documented severe acute respiratory syndrome who required oxygen, HCQ did not show an obvious therapeutic effect. Additionally, eight patients in the HCQ group (10%) experienced electrocardiographic modifications that required discontinuation of treatment [104]. Despite the controversial results of these clinical trials, frequent side effects of CQ and HCQ, for example, worsening vision, nausea, digestive disorders and potential heart failure and even death, have hindered the wide application of these drugs [105]. Moreover, the results of a clinical trial conducted by Rosenberg et al., which involved 1438 COVID-19 patients, showed that compared with neither treatment, treatment with HCQ alone or combined with azithromycin was not significantly associated with differences in mortality [96]. ...
Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro
1
2020
... Chloroquine (CQ) and its derivative hydroxychloroquine (HCQ) have the ability to induce alkalization, which functionally prevents the induction and accumulation of beta-galactosidase (β-Gal), known as a marker of senescence [97]. CQ and HCQ are widely used antimalarial and antiviral drugs and have recently received much attention as potential treatments for COVID-19 [98].CQ was recently demonstrated as an inhibitor ofSARS-CoV-2 in vitro, and the hydroxylated form, HCQ, has been proven to limit the replication of SARS-CoV-2 in vitro [99, 100]. Huang et al. found that CQ had a slight advantage over lopinavir/ritonavir in COVID-19 patients [101]. HCQ can also specifically inhibit the replication of SARS-CoV by interfering with the glycosylation of ACE2 [102]. Therefore, HCQ has been widely suggested as a potential treatment for patients with SARS-CoV-2 infection. A number of clinical trials have been conducted to explore the efficacies of CQ and HCQ. According to a small open-label nonrandomized clinical trial, HCQ treatment was significantly associated with viral load reduction in COVID-19 patients, and its efficacy could be reinforced by azithromycin [103]. However, according to a newly published comparative observational study among 181 COVID-19 patients with documented severe acute respiratory syndrome who required oxygen, HCQ did not show an obvious therapeutic effect. Additionally, eight patients in the HCQ group (10%) experienced electrocardiographic modifications that required discontinuation of treatment [104]. Despite the controversial results of these clinical trials, frequent side effects of CQ and HCQ, for example, worsening vision, nausea, digestive disorders and potential heart failure and even death, have hindered the wide application of these drugs [105]. Moreover, the results of a clinical trial conducted by Rosenberg et al., which involved 1438 COVID-19 patients, showed that compared with neither treatment, treatment with HCQ alone or combined with azithromycin was not significantly associated with differences in mortality [96]. ...
Treating COVID-19 with Chloroquine
1
2020
... Chloroquine (CQ) and its derivative hydroxychloroquine (HCQ) have the ability to induce alkalization, which functionally prevents the induction and accumulation of beta-galactosidase (β-Gal), known as a marker of senescence [97]. CQ and HCQ are widely used antimalarial and antiviral drugs and have recently received much attention as potential treatments for COVID-19 [98].CQ was recently demonstrated as an inhibitor ofSARS-CoV-2 in vitro, and the hydroxylated form, HCQ, has been proven to limit the replication of SARS-CoV-2 in vitro [99, 100]. Huang et al. found that CQ had a slight advantage over lopinavir/ritonavir in COVID-19 patients [101]. HCQ can also specifically inhibit the replication of SARS-CoV by interfering with the glycosylation of ACE2 [102]. Therefore, HCQ has been widely suggested as a potential treatment for patients with SARS-CoV-2 infection. A number of clinical trials have been conducted to explore the efficacies of CQ and HCQ. According to a small open-label nonrandomized clinical trial, HCQ treatment was significantly associated with viral load reduction in COVID-19 patients, and its efficacy could be reinforced by azithromycin [103]. However, according to a newly published comparative observational study among 181 COVID-19 patients with documented severe acute respiratory syndrome who required oxygen, HCQ did not show an obvious therapeutic effect. Additionally, eight patients in the HCQ group (10%) experienced electrocardiographic modifications that required discontinuation of treatment [104]. Despite the controversial results of these clinical trials, frequent side effects of CQ and HCQ, for example, worsening vision, nausea, digestive disorders and potential heart failure and even death, have hindered the wide application of these drugs [105]. Moreover, the results of a clinical trial conducted by Rosenberg et al., which involved 1438 COVID-19 patients, showed that compared with neither treatment, treatment with HCQ alone or combined with azithromycin was not significantly associated with differences in mortality [96]. ...
Chloroquine is a potent inhibitor of SARS coronavirus infection and spread
1
2005
... Chloroquine (CQ) and its derivative hydroxychloroquine (HCQ) have the ability to induce alkalization, which functionally prevents the induction and accumulation of beta-galactosidase (β-Gal), known as a marker of senescence [97]. CQ and HCQ are widely used antimalarial and antiviral drugs and have recently received much attention as potential treatments for COVID-19 [98].CQ was recently demonstrated as an inhibitor ofSARS-CoV-2 in vitro, and the hydroxylated form, HCQ, has been proven to limit the replication of SARS-CoV-2 in vitro [99, 100]. Huang et al. found that CQ had a slight advantage over lopinavir/ritonavir in COVID-19 patients [101]. HCQ can also specifically inhibit the replication of SARS-CoV by interfering with the glycosylation of ACE2 [102]. Therefore, HCQ has been widely suggested as a potential treatment for patients with SARS-CoV-2 infection. A number of clinical trials have been conducted to explore the efficacies of CQ and HCQ. According to a small open-label nonrandomized clinical trial, HCQ treatment was significantly associated with viral load reduction in COVID-19 patients, and its efficacy could be reinforced by azithromycin [103]. However, according to a newly published comparative observational study among 181 COVID-19 patients with documented severe acute respiratory syndrome who required oxygen, HCQ did not show an obvious therapeutic effect. Additionally, eight patients in the HCQ group (10%) experienced electrocardiographic modifications that required discontinuation of treatment [104]. Despite the controversial results of these clinical trials, frequent side effects of CQ and HCQ, for example, worsening vision, nausea, digestive disorders and potential heart failure and even death, have hindered the wide application of these drugs [105]. Moreover, the results of a clinical trial conducted by Rosenberg et al., which involved 1438 COVID-19 patients, showed that compared with neither treatment, treatment with HCQ alone or combined with azithromycin was not significantly associated with differences in mortality [96]. ...
Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open-label non-randomized clinical trial
1
2020
... Chloroquine (CQ) and its derivative hydroxychloroquine (HCQ) have the ability to induce alkalization, which functionally prevents the induction and accumulation of beta-galactosidase (β-Gal), known as a marker of senescence [97]. CQ and HCQ are widely used antimalarial and antiviral drugs and have recently received much attention as potential treatments for COVID-19 [98].CQ was recently demonstrated as an inhibitor ofSARS-CoV-2 in vitro, and the hydroxylated form, HCQ, has been proven to limit the replication of SARS-CoV-2 in vitro [99, 100]. Huang et al. found that CQ had a slight advantage over lopinavir/ritonavir in COVID-19 patients [101]. HCQ can also specifically inhibit the replication of SARS-CoV by interfering with the glycosylation of ACE2 [102]. Therefore, HCQ has been widely suggested as a potential treatment for patients with SARS-CoV-2 infection. A number of clinical trials have been conducted to explore the efficacies of CQ and HCQ. According to a small open-label nonrandomized clinical trial, HCQ treatment was significantly associated with viral load reduction in COVID-19 patients, and its efficacy could be reinforced by azithromycin [103]. However, according to a newly published comparative observational study among 181 COVID-19 patients with documented severe acute respiratory syndrome who required oxygen, HCQ did not show an obvious therapeutic effect. Additionally, eight patients in the HCQ group (10%) experienced electrocardiographic modifications that required discontinuation of treatment [104]. Despite the controversial results of these clinical trials, frequent side effects of CQ and HCQ, for example, worsening vision, nausea, digestive disorders and potential heart failure and even death, have hindered the wide application of these drugs [105]. Moreover, the results of a clinical trial conducted by Rosenberg et al., which involved 1438 COVID-19 patients, showed that compared with neither treatment, treatment with HCQ alone or combined with azithromycin was not significantly associated with differences in mortality [96]. ...
Clinical efficacy of hydroxychloroquine in patients with covid-19 pneumonia who require oxygen: observational comparative study using routine care data
1
2020
... Chloroquine (CQ) and its derivative hydroxychloroquine (HCQ) have the ability to induce alkalization, which functionally prevents the induction and accumulation of beta-galactosidase (β-Gal), known as a marker of senescence [97]. CQ and HCQ are widely used antimalarial and antiviral drugs and have recently received much attention as potential treatments for COVID-19 [98].CQ was recently demonstrated as an inhibitor ofSARS-CoV-2 in vitro, and the hydroxylated form, HCQ, has been proven to limit the replication of SARS-CoV-2 in vitro [99, 100]. Huang et al. found that CQ had a slight advantage over lopinavir/ritonavir in COVID-19 patients [101]. HCQ can also specifically inhibit the replication of SARS-CoV by interfering with the glycosylation of ACE2 [102]. Therefore, HCQ has been widely suggested as a potential treatment for patients with SARS-CoV-2 infection. A number of clinical trials have been conducted to explore the efficacies of CQ and HCQ. According to a small open-label nonrandomized clinical trial, HCQ treatment was significantly associated with viral load reduction in COVID-19 patients, and its efficacy could be reinforced by azithromycin [103]. However, according to a newly published comparative observational study among 181 COVID-19 patients with documented severe acute respiratory syndrome who required oxygen, HCQ did not show an obvious therapeutic effect. Additionally, eight patients in the HCQ group (10%) experienced electrocardiographic modifications that required discontinuation of treatment [104]. Despite the controversial results of these clinical trials, frequent side effects of CQ and HCQ, for example, worsening vision, nausea, digestive disorders and potential heart failure and even death, have hindered the wide application of these drugs [105]. Moreover, the results of a clinical trial conducted by Rosenberg et al., which involved 1438 COVID-19 patients, showed that compared with neither treatment, treatment with HCQ alone or combined with azithromycin was not significantly associated with differences in mortality [96]. ...
Recent progress and challenges in drug development against COVID-19 coronavirus (SARS-CoV-2) - an update on the status
1
2020
... Chloroquine (CQ) and its derivative hydroxychloroquine (HCQ) have the ability to induce alkalization, which functionally prevents the induction and accumulation of beta-galactosidase (β-Gal), known as a marker of senescence [97]. CQ and HCQ are widely used antimalarial and antiviral drugs and have recently received much attention as potential treatments for COVID-19 [98].CQ was recently demonstrated as an inhibitor ofSARS-CoV-2 in vitro, and the hydroxylated form, HCQ, has been proven to limit the replication of SARS-CoV-2 in vitro [99, 100]. Huang et al. found that CQ had a slight advantage over lopinavir/ritonavir in COVID-19 patients [101]. HCQ can also specifically inhibit the replication of SARS-CoV by interfering with the glycosylation of ACE2 [102]. Therefore, HCQ has been widely suggested as a potential treatment for patients with SARS-CoV-2 infection. A number of clinical trials have been conducted to explore the efficacies of CQ and HCQ. According to a small open-label nonrandomized clinical trial, HCQ treatment was significantly associated with viral load reduction in COVID-19 patients, and its efficacy could be reinforced by azithromycin [103]. However, according to a newly published comparative observational study among 181 COVID-19 patients with documented severe acute respiratory syndrome who required oxygen, HCQ did not show an obvious therapeutic effect. Additionally, eight patients in the HCQ group (10%) experienced electrocardiographic modifications that required discontinuation of treatment [104]. Despite the controversial results of these clinical trials, frequent side effects of CQ and HCQ, for example, worsening vision, nausea, digestive disorders and potential heart failure and even death, have hindered the wide application of these drugs [105]. Moreover, the results of a clinical trial conducted by Rosenberg et al., which involved 1438 COVID-19 patients, showed that compared with neither treatment, treatment with HCQ alone or combined with azithromycin was not significantly associated with differences in mortality [96]. ...
Rapamycin decelerates cellular senescence
1
2009
... Rapamycin is widely known as a key anti-aging drug and prevents the progression of senescence in human cell lines and animal models [106-108]. Rapamycin acts as an inhibitor of protein synthesis, inhibiting cytokine expression and viral replication [109]. In elderly patients, especially those with CHD or reduced T-cell counts, rapamycin can significantly reduce the expression of the serum senescence marker IL-6 [110]. As a candidate for potential use in COVID-19, rapamycin may prevent progression to severe forms of COVID-19 by downregulating the IL-6 pathway and reducing the number of senescent T-cells through the mTOR-NLRP3-IL-1β axis at the early stage of cytokine storms [111, 112]. Conversely, rapamycin is suggested as a novel intervention strategy beyond vaccines to prevent severe symptoms in COVID-19 [113]. Therefore, conducting clinical trials for rapamycin to prevent and treat the severity of COVID-19 patients, especially elderly patients, is strongly recommended. ...
Long term rapamycin treatment improves mitochondrial DNA quality in aging mice
0
2018
Rapamycin: An InhibiTOR of Aging Emerges From the Soil of Easter Island
1
2016
... Rapamycin is widely known as a key anti-aging drug and prevents the progression of senescence in human cell lines and animal models [106-108]. Rapamycin acts as an inhibitor of protein synthesis, inhibiting cytokine expression and viral replication [109]. In elderly patients, especially those with CHD or reduced T-cell counts, rapamycin can significantly reduce the expression of the serum senescence marker IL-6 [110]. As a candidate for potential use in COVID-19, rapamycin may prevent progression to severe forms of COVID-19 by downregulating the IL-6 pathway and reducing the number of senescent T-cells through the mTOR-NLRP3-IL-1β axis at the early stage of cytokine storms [111, 112]. Conversely, rapamycin is suggested as a novel intervention strategy beyond vaccines to prevent severe symptoms in COVID-19 [113]. Therefore, conducting clinical trials for rapamycin to prevent and treat the severity of COVID-19 patients, especially elderly patients, is strongly recommended. ...
COVID-19 and chronological aging:
1
2020
... Rapamycin is widely known as a key anti-aging drug and prevents the progression of senescence in human cell lines and animal models [106-108]. Rapamycin acts as an inhibitor of protein synthesis, inhibiting cytokine expression and viral replication [109]. In elderly patients, especially those with CHD or reduced T-cell counts, rapamycin can significantly reduce the expression of the serum senescence marker IL-6 [110]. As a candidate for potential use in COVID-19, rapamycin may prevent progression to severe forms of COVID-19 by downregulating the IL-6 pathway and reducing the number of senescent T-cells through the mTOR-NLRP3-IL-1β axis at the early stage of cytokine storms [111, 112]. Conversely, rapamycin is suggested as a novel intervention strategy beyond vaccines to prevent severe symptoms in COVID-19 [113]. Therefore, conducting clinical trials for rapamycin to prevent and treat the severity of COVID-19 patients, especially elderly patients, is strongly recommended. ...
Effect of Low-Dose Rapamycin on Senescence Markers and Physical Functioning in Older Adults with Coronary Artery Disease: Results of a Pilot Study
1
2016
... Rapamycin is widely known as a key anti-aging drug and prevents the progression of senescence in human cell lines and animal models [106-108]. Rapamycin acts as an inhibitor of protein synthesis, inhibiting cytokine expression and viral replication [109]. In elderly patients, especially those with CHD or reduced T-cell counts, rapamycin can significantly reduce the expression of the serum senescence marker IL-6 [110]. As a candidate for potential use in COVID-19, rapamycin may prevent progression to severe forms of COVID-19 by downregulating the IL-6 pathway and reducing the number of senescent T-cells through the mTOR-NLRP3-IL-1β axis at the early stage of cytokine storms [111, 112]. Conversely, rapamycin is suggested as a novel intervention strategy beyond vaccines to prevent severe symptoms in COVID-19 [113]. Therefore, conducting clinical trials for rapamycin to prevent and treat the severity of COVID-19 patients, especially elderly patients, is strongly recommended. ...
Network-based drug repurposing for novel coronavirus 2019-nCoV/SARS-CoV-2
1
2020
... Rapamycin is widely known as a key anti-aging drug and prevents the progression of senescence in human cell lines and animal models [106-108]. Rapamycin acts as an inhibitor of protein synthesis, inhibiting cytokine expression and viral replication [109]. In elderly patients, especially those with CHD or reduced T-cell counts, rapamycin can significantly reduce the expression of the serum senescence marker IL-6 [110]. As a candidate for potential use in COVID-19, rapamycin may prevent progression to severe forms of COVID-19 by downregulating the IL-6 pathway and reducing the number of senescent T-cells through the mTOR-NLRP3-IL-1β axis at the early stage of cytokine storms [111, 112]. Conversely, rapamycin is suggested as a novel intervention strategy beyond vaccines to prevent severe symptoms in COVID-19 [113]. Therefore, conducting clinical trials for rapamycin to prevent and treat the severity of COVID-19 patients, especially elderly patients, is strongly recommended. ...
Targeting T-cell senescence and cytokine storm with rapamycin to prevent severe progression in COVID-19
1
2020
... Rapamycin is widely known as a key anti-aging drug and prevents the progression of senescence in human cell lines and animal models [106-108]. Rapamycin acts as an inhibitor of protein synthesis, inhibiting cytokine expression and viral replication [109]. In elderly patients, especially those with CHD or reduced T-cell counts, rapamycin can significantly reduce the expression of the serum senescence marker IL-6 [110]. As a candidate for potential use in COVID-19, rapamycin may prevent progression to severe forms of COVID-19 by downregulating the IL-6 pathway and reducing the number of senescent T-cells through the mTOR-NLRP3-IL-1β axis at the early stage of cytokine storms [111, 112]. Conversely, rapamycin is suggested as a novel intervention strategy beyond vaccines to prevent severe symptoms in COVID-19 [113]. Therefore, conducting clinical trials for rapamycin to prevent and treat the severity of COVID-19 patients, especially elderly patients, is strongly recommended. ...
Immunoregulation with mTOR inhibitors to prevent COVID-19 severity: A novel intervention strategy beyond vaccines and specific antiviral medicines
1
2020
... Rapamycin is widely known as a key anti-aging drug and prevents the progression of senescence in human cell lines and animal models [106-108]. Rapamycin acts as an inhibitor of protein synthesis, inhibiting cytokine expression and viral replication [109]. In elderly patients, especially those with CHD or reduced T-cell counts, rapamycin can significantly reduce the expression of the serum senescence marker IL-6 [110]. As a candidate for potential use in COVID-19, rapamycin may prevent progression to severe forms of COVID-19 by downregulating the IL-6 pathway and reducing the number of senescent T-cells through the mTOR-NLRP3-IL-1β axis at the early stage of cytokine storms [111, 112]. Conversely, rapamycin is suggested as a novel intervention strategy beyond vaccines to prevent severe symptoms in COVID-19 [113]. Therefore, conducting clinical trials for rapamycin to prevent and treat the severity of COVID-19 patients, especially elderly patients, is strongly recommended. ...
Activation of angiotensin-converting enzyme 2 (ACE2) attenuates allergic airway inflammation in rat asthma model
1
2016
... Some researchers have suggested that SARS-CoV-2 induces initial damage effects by downregulating ACE2 expression and blocking ACE2-mediated activity and activating ACE2 may be much more efficacious. Accumulating evidence has illustrated that the activation of ACE2 could be a positive treatment method. ACE2 activators are purported to have two therapeutic effects: avoiding the binding of the S protein of SARS-CoV-2 to ACE2 and promoting the protective effects of different organs, preventing lung injury and fibrosis [34, 114, 115].ACE2 activators, such as diminazene aceturate, are recommended for application in COVID-19 patients [34]. ...
Original Research: ACE2 activator associated with physical exercise potentiates the reduction of pulmonary fibrosis
1
2017
... Some researchers have suggested that SARS-CoV-2 induces initial damage effects by downregulating ACE2 expression and blocking ACE2-mediated activity and activating ACE2 may be much more efficacious. Accumulating evidence has illustrated that the activation of ACE2 could be a positive treatment method. ACE2 activators are purported to have two therapeutic effects: avoiding the binding of the S protein of SARS-CoV-2 to ACE2 and promoting the protective effects of different organs, preventing lung injury and fibrosis [34, 114, 115].ACE2 activators, such as diminazene aceturate, are recommended for application in COVID-19 patients [34]. ...
Organ-protective effect of angiotensin-converting enzyme 2 and its effect on the prognosis of COVID-19
1
2020
... However, due to the positive-feedback loop between virus infection and ACE2 expression, some researchers have suggested the use of ACE2 inhibitors to block SARS-CoV-2 infection. Considering the role of ACE2 in maintaining organ functioning, especially in the lungs, the clinical application of ACE2 inhibitors in COVID-19 is under question [116]. The findings regardingACE2 have sparked a debate regarding the potential use of angiotensin-converting enzyme inhibitors (ACEIs) and AngII receptor blockers (ARBs) among elderly COVID-19 patients in the context of the pandemic [117]. However, after reviewing published relevant animal, in vitro and clinical studies, Chung et al. announced that the results did not show a higher risk of infection with ACEI or ARB use [118]. Considering the contradictory hypotheses and lack of scientific evidence and clinical data worldwide, the European Society of Cardiology and the American College of Cardiology recommended the continuation of ACEIs or ARBs for COVID-19 patients who were already taking these medicines [119, 120]. ...
Renin-Angiotensin-Aldosterone System Inhibitors in Patients with Covid-19
1
2020
... However, due to the positive-feedback loop between virus infection and ACE2 expression, some researchers have suggested the use of ACE2 inhibitors to block SARS-CoV-2 infection. Considering the role of ACE2 in maintaining organ functioning, especially in the lungs, the clinical application of ACE2 inhibitors in COVID-19 is under question [116]. The findings regardingACE2 have sparked a debate regarding the potential use of angiotensin-converting enzyme inhibitors (ACEIs) and AngII receptor blockers (ARBs) among elderly COVID-19 patients in the context of the pandemic [117]. However, after reviewing published relevant animal, in vitro and clinical studies, Chung et al. announced that the results did not show a higher risk of infection with ACEI or ARB use [118]. Considering the contradictory hypotheses and lack of scientific evidence and clinical data worldwide, the European Society of Cardiology and the American College of Cardiology recommended the continuation of ACEIs or ARBs for COVID-19 patients who were already taking these medicines [119, 120]. ...
SARS-CoV-2 and ACE2: The biology and clinical data settling the ARB and ACEI controversy
1
2020
... However, due to the positive-feedback loop between virus infection and ACE2 expression, some researchers have suggested the use of ACE2 inhibitors to block SARS-CoV-2 infection. Considering the role of ACE2 in maintaining organ functioning, especially in the lungs, the clinical application of ACE2 inhibitors in COVID-19 is under question [116]. The findings regardingACE2 have sparked a debate regarding the potential use of angiotensin-converting enzyme inhibitors (ACEIs) and AngII receptor blockers (ARBs) among elderly COVID-19 patients in the context of the pandemic [117]. However, after reviewing published relevant animal, in vitro and clinical studies, Chung et al. announced that the results did not show a higher risk of infection with ACEI or ARB use [118]. Considering the contradictory hypotheses and lack of scientific evidence and clinical data worldwide, the European Society of Cardiology and the American College of Cardiology recommended the continuation of ACEIs or ARBs for COVID-19 patients who were already taking these medicines [119, 120]. ...
Outcomes in Patients with COVID-19 Infection Taking ACEI/ARB
1
2020
... However, due to the positive-feedback loop between virus infection and ACE2 expression, some researchers have suggested the use of ACE2 inhibitors to block SARS-CoV-2 infection. Considering the role of ACE2 in maintaining organ functioning, especially in the lungs, the clinical application of ACE2 inhibitors in COVID-19 is under question [116]. The findings regardingACE2 have sparked a debate regarding the potential use of angiotensin-converting enzyme inhibitors (ACEIs) and AngII receptor blockers (ARBs) among elderly COVID-19 patients in the context of the pandemic [117]. However, after reviewing published relevant animal, in vitro and clinical studies, Chung et al. announced that the results did not show a higher risk of infection with ACEI or ARB use [118]. Considering the contradictory hypotheses and lack of scientific evidence and clinical data worldwide, the European Society of Cardiology and the American College of Cardiology recommended the continuation of ACEIs or ARBs for COVID-19 patients who were already taking these medicines [119, 120]. ...
COVID-19: The Influence of ACE Genotype and ACE-I and ARBs on the Course of SARS-CoV-2 Infection in Elderly Patients
1
2020
... However, due to the positive-feedback loop between virus infection and ACE2 expression, some researchers have suggested the use of ACE2 inhibitors to block SARS-CoV-2 infection. Considering the role of ACE2 in maintaining organ functioning, especially in the lungs, the clinical application of ACE2 inhibitors in COVID-19 is under question [116]. The findings regardingACE2 have sparked a debate regarding the potential use of angiotensin-converting enzyme inhibitors (ACEIs) and AngII receptor blockers (ARBs) among elderly COVID-19 patients in the context of the pandemic [117]. However, after reviewing published relevant animal, in vitro and clinical studies, Chung et al. announced that the results did not show a higher risk of infection with ACEI or ARB use [118]. Considering the contradictory hypotheses and lack of scientific evidence and clinical data worldwide, the European Society of Cardiology and the American College of Cardiology recommended the continuation of ACEIs or ARBs for COVID-19 patients who were already taking these medicines [119, 120]. ...
A pilot clinical trial of recombinant human angiotensin-converting enzyme 2 in acute respiratory distress syndrome
1
2017
... Human recombinant soluble ACE2 (hrsACE2) is an FDA-approved treatment, with a 2017 phase II trial for ARDS [121]. Circulating soluble ACE2 can bind to SARS-CoV-2 but is unable to inhibit cell infection [122]. According to Monteil et al., clinical grade hrsACE2 reduces SARS-CoV-2 recovery from Vero cells by 1,000-5,000 times, demonstrating that hrsACE2 can not only block SARS-CoV-2 infection but also protect against lung injury, suggesting a possible therapeutic approach [123]. ...
Renin-angiotensin-aldosterone system and COVID-19 infection
1
2020
... Human recombinant soluble ACE2 (hrsACE2) is an FDA-approved treatment, with a 2017 phase II trial for ARDS [121]. Circulating soluble ACE2 can bind to SARS-CoV-2 but is unable to inhibit cell infection [122]. According to Monteil et al., clinical grade hrsACE2 reduces SARS-CoV-2 recovery from Vero cells by 1,000-5,000 times, demonstrating that hrsACE2 can not only block SARS-CoV-2 infection but also protect against lung injury, suggesting a possible therapeutic approach [123]. ...
Inhibition of SARS-CoV-2 Infections in Engineered Human Tissues Using Clinical-Grade Soluble Human ACE2
1
2020
... Human recombinant soluble ACE2 (hrsACE2) is an FDA-approved treatment, with a 2017 phase II trial for ARDS [121]. Circulating soluble ACE2 can bind to SARS-CoV-2 but is unable to inhibit cell infection [122]. According to Monteil et al., clinical grade hrsACE2 reduces SARS-CoV-2 recovery from Vero cells by 1,000-5,000 times, demonstrating that hrsACE2 can not only block SARS-CoV-2 infection but also protect against lung injury, suggesting a possible therapeutic approach [123]. ...
COVID-19 infection: the perspectives on immune responses
1
2020
... The clinical immune response to SARS-CoV-2 can be divided into 2 phases: an earlier phase of elimination by antiviral adaptive immunity and a later phase of damaged alveolar cells triggering innate inflammation [124]. According to Chen et al., the occurrence of ARDS may be associated with the later immune phase, and treatment to reduce inflammation during that phase may help reduce lung damage. CD26 inhibitors may potentially act to regulate an overactive immune reaction and prevent devastating lung injury [125]. In a mouse model of ARDS, which is the main cause of death in COVID-19 patients, CD26 inhibition by sitagliptin alleviated histological findings of lung injury by inhibiting the expression of IL-1β, TNF-α, and IL-6[126]. Birnbaum et al. reported that saxagliptin-mediated DPP4 inhibition could attenuate diabetes mellitus (DM) -induced activation of nod-like receptor family pyrin domain-containing 3 (NLRP3) inflammatory bodies, thus reducing serum CRP, TNF-α, IL-1β, IL-18 and IL-6 levels [127]. CD26 inhibitors, including sitagliptin, alogliptin, vildagliptin, saxagliptin, and linagliptin, are a class of drugs used effectively in the treatment of type 2 diabetes, which has demonstrated safety in elderly patients. These drugs have similar effects by binding to essentially the same catalytic site [128]. Research has shown that the administration of linagliptin can lead to a decrease in the concentration of proinflammatory factors, especially TNF-α and IL-6 [66]. Moreover, mathematical modeling has shown that the spread of MERS-CoV infection can be controlled by inhibiting the expression of CD26, with similar efficiency in SARS-CoV-2 infection [129]. Since the expression of CD26 is closely related to the pathogenesis and severity of COVID-19, CD26 inhibitors have recently been proposed as potential drugsagainst COVID-19 [130]. However, despite laboratory verification and theoretical feasibility, the actual efficacies of CD26 inhibitors in COVID-19 still require verification in further clinical trials. ...
Role of Dipeptidyl Peptidase 4 Inhibitors in Diabetic Patients with Coronavirus-19 Infection. J
1
2020
... The clinical immune response to SARS-CoV-2 can be divided into 2 phases: an earlier phase of elimination by antiviral adaptive immunity and a later phase of damaged alveolar cells triggering innate inflammation [124]. According to Chen et al., the occurrence of ARDS may be associated with the later immune phase, and treatment to reduce inflammation during that phase may help reduce lung damage. CD26 inhibitors may potentially act to regulate an overactive immune reaction and prevent devastating lung injury [125]. In a mouse model of ARDS, which is the main cause of death in COVID-19 patients, CD26 inhibition by sitagliptin alleviated histological findings of lung injury by inhibiting the expression of IL-1β, TNF-α, and IL-6[126]. Birnbaum et al. reported that saxagliptin-mediated DPP4 inhibition could attenuate diabetes mellitus (DM) -induced activation of nod-like receptor family pyrin domain-containing 3 (NLRP3) inflammatory bodies, thus reducing serum CRP, TNF-α, IL-1β, IL-18 and IL-6 levels [127]. CD26 inhibitors, including sitagliptin, alogliptin, vildagliptin, saxagliptin, and linagliptin, are a class of drugs used effectively in the treatment of type 2 diabetes, which has demonstrated safety in elderly patients. These drugs have similar effects by binding to essentially the same catalytic site [128]. Research has shown that the administration of linagliptin can lead to a decrease in the concentration of proinflammatory factors, especially TNF-α and IL-6 [66]. Moreover, mathematical modeling has shown that the spread of MERS-CoV infection can be controlled by inhibiting the expression of CD26, with similar efficiency in SARS-CoV-2 infection [129]. Since the expression of CD26 is closely related to the pathogenesis and severity of COVID-19, CD26 inhibitors have recently been proposed as potential drugsagainst COVID-19 [130]. However, despite laboratory verification and theoretical feasibility, the actual efficacies of CD26 inhibitors in COVID-19 still require verification in further clinical trials. ...
DPP4 inhibition by sitagliptin attenuates LPS-induced lung injury in mice
1
2018
... The clinical immune response to SARS-CoV-2 can be divided into 2 phases: an earlier phase of elimination by antiviral adaptive immunity and a later phase of damaged alveolar cells triggering innate inflammation [124]. According to Chen et al., the occurrence of ARDS may be associated with the later immune phase, and treatment to reduce inflammation during that phase may help reduce lung damage. CD26 inhibitors may potentially act to regulate an overactive immune reaction and prevent devastating lung injury [125]. In a mouse model of ARDS, which is the main cause of death in COVID-19 patients, CD26 inhibition by sitagliptin alleviated histological findings of lung injury by inhibiting the expression of IL-1β, TNF-α, and IL-6[126]. Birnbaum et al. reported that saxagliptin-mediated DPP4 inhibition could attenuate diabetes mellitus (DM) -induced activation of nod-like receptor family pyrin domain-containing 3 (NLRP3) inflammatory bodies, thus reducing serum CRP, TNF-α, IL-1β, IL-18 and IL-6 levels [127]. CD26 inhibitors, including sitagliptin, alogliptin, vildagliptin, saxagliptin, and linagliptin, are a class of drugs used effectively in the treatment of type 2 diabetes, which has demonstrated safety in elderly patients. These drugs have similar effects by binding to essentially the same catalytic site [128]. Research has shown that the administration of linagliptin can lead to a decrease in the concentration of proinflammatory factors, especially TNF-α and IL-6 [66]. Moreover, mathematical modeling has shown that the spread of MERS-CoV infection can be controlled by inhibiting the expression of CD26, with similar efficiency in SARS-CoV-2 infection [129]. Since the expression of CD26 is closely related to the pathogenesis and severity of COVID-19, CD26 inhibitors have recently been proposed as potential drugsagainst COVID-19 [130]. However, despite laboratory verification and theoretical feasibility, the actual efficacies of CD26 inhibitors in COVID-19 still require verification in further clinical trials. ...
Dipeptidyl peptidase-4 inhibition by Saxagliptin prevents inflammation and renal injury by targeting the Nlrp3/ASC inflammasome
1
2016
... The clinical immune response to SARS-CoV-2 can be divided into 2 phases: an earlier phase of elimination by antiviral adaptive immunity and a later phase of damaged alveolar cells triggering innate inflammation [124]. According to Chen et al., the occurrence of ARDS may be associated with the later immune phase, and treatment to reduce inflammation during that phase may help reduce lung damage. CD26 inhibitors may potentially act to regulate an overactive immune reaction and prevent devastating lung injury [125]. In a mouse model of ARDS, which is the main cause of death in COVID-19 patients, CD26 inhibition by sitagliptin alleviated histological findings of lung injury by inhibiting the expression of IL-1β, TNF-α, and IL-6[126]. Birnbaum et al. reported that saxagliptin-mediated DPP4 inhibition could attenuate diabetes mellitus (DM) -induced activation of nod-like receptor family pyrin domain-containing 3 (NLRP3) inflammatory bodies, thus reducing serum CRP, TNF-α, IL-1β, IL-18 and IL-6 levels [127]. CD26 inhibitors, including sitagliptin, alogliptin, vildagliptin, saxagliptin, and linagliptin, are a class of drugs used effectively in the treatment of type 2 diabetes, which has demonstrated safety in elderly patients. These drugs have similar effects by binding to essentially the same catalytic site [128]. Research has shown that the administration of linagliptin can lead to a decrease in the concentration of proinflammatory factors, especially TNF-α and IL-6 [66]. Moreover, mathematical modeling has shown that the spread of MERS-CoV infection can be controlled by inhibiting the expression of CD26, with similar efficiency in SARS-CoV-2 infection [129]. Since the expression of CD26 is closely related to the pathogenesis and severity of COVID-19, CD26 inhibitors have recently been proposed as potential drugsagainst COVID-19 [130]. However, despite laboratory verification and theoretical feasibility, the actual efficacies of CD26 inhibitors in COVID-19 still require verification in further clinical trials. ...
A comparative study of the binding properties, dipeptidyl peptidase-4 (DPP-4) inhibitory activity and glucose-lowering efficacy of the DPP-4 inhibitors alogliptin, linagliptin, saxagliptin, sitagliptin and vildagliptin in mice
1
2018
... The clinical immune response to SARS-CoV-2 can be divided into 2 phases: an earlier phase of elimination by antiviral adaptive immunity and a later phase of damaged alveolar cells triggering innate inflammation [124]. According to Chen et al., the occurrence of ARDS may be associated with the later immune phase, and treatment to reduce inflammation during that phase may help reduce lung damage. CD26 inhibitors may potentially act to regulate an overactive immune reaction and prevent devastating lung injury [125]. In a mouse model of ARDS, which is the main cause of death in COVID-19 patients, CD26 inhibition by sitagliptin alleviated histological findings of lung injury by inhibiting the expression of IL-1β, TNF-α, and IL-6[126]. Birnbaum et al. reported that saxagliptin-mediated DPP4 inhibition could attenuate diabetes mellitus (DM) -induced activation of nod-like receptor family pyrin domain-containing 3 (NLRP3) inflammatory bodies, thus reducing serum CRP, TNF-α, IL-1β, IL-18 and IL-6 levels [127]. CD26 inhibitors, including sitagliptin, alogliptin, vildagliptin, saxagliptin, and linagliptin, are a class of drugs used effectively in the treatment of type 2 diabetes, which has demonstrated safety in elderly patients. These drugs have similar effects by binding to essentially the same catalytic site [128]. Research has shown that the administration of linagliptin can lead to a decrease in the concentration of proinflammatory factors, especially TNF-α and IL-6 [66]. Moreover, mathematical modeling has shown that the spread of MERS-CoV infection can be controlled by inhibiting the expression of CD26, with similar efficiency in SARS-CoV-2 infection [129]. Since the expression of CD26 is closely related to the pathogenesis and severity of COVID-19, CD26 inhibitors have recently been proposed as potential drugsagainst COVID-19 [130]. However, despite laboratory verification and theoretical feasibility, the actual efficacies of CD26 inhibitors in COVID-19 still require verification in further clinical trials. ...
A Novel Dynamic Model Describing the Spread of the MERS-CoV and the Expression of Dipeptidyl Peptidase 4
1
2017
... The clinical immune response to SARS-CoV-2 can be divided into 2 phases: an earlier phase of elimination by antiviral adaptive immunity and a later phase of damaged alveolar cells triggering innate inflammation [124]. According to Chen et al., the occurrence of ARDS may be associated with the later immune phase, and treatment to reduce inflammation during that phase may help reduce lung damage. CD26 inhibitors may potentially act to regulate an overactive immune reaction and prevent devastating lung injury [125]. In a mouse model of ARDS, which is the main cause of death in COVID-19 patients, CD26 inhibition by sitagliptin alleviated histological findings of lung injury by inhibiting the expression of IL-1β, TNF-α, and IL-6[126]. Birnbaum et al. reported that saxagliptin-mediated DPP4 inhibition could attenuate diabetes mellitus (DM) -induced activation of nod-like receptor family pyrin domain-containing 3 (NLRP3) inflammatory bodies, thus reducing serum CRP, TNF-α, IL-1β, IL-18 and IL-6 levels [127]. CD26 inhibitors, including sitagliptin, alogliptin, vildagliptin, saxagliptin, and linagliptin, are a class of drugs used effectively in the treatment of type 2 diabetes, which has demonstrated safety in elderly patients. These drugs have similar effects by binding to essentially the same catalytic site [128]. Research has shown that the administration of linagliptin can lead to a decrease in the concentration of proinflammatory factors, especially TNF-α and IL-6 [66]. Moreover, mathematical modeling has shown that the spread of MERS-CoV infection can be controlled by inhibiting the expression of CD26, with similar efficiency in SARS-CoV-2 infection [129]. Since the expression of CD26 is closely related to the pathogenesis and severity of COVID-19, CD26 inhibitors have recently been proposed as potential drugsagainst COVID-19 [130]. However, despite laboratory verification and theoretical feasibility, the actual efficacies of CD26 inhibitors in COVID-19 still require verification in further clinical trials. ...
COVID-19 and diabetes: Can DPP4 inhibition play a role?
1
2020
... The clinical immune response to SARS-CoV-2 can be divided into 2 phases: an earlier phase of elimination by antiviral adaptive immunity and a later phase of damaged alveolar cells triggering innate inflammation [124]. According to Chen et al., the occurrence of ARDS may be associated with the later immune phase, and treatment to reduce inflammation during that phase may help reduce lung damage. CD26 inhibitors may potentially act to regulate an overactive immune reaction and prevent devastating lung injury [125]. In a mouse model of ARDS, which is the main cause of death in COVID-19 patients, CD26 inhibition by sitagliptin alleviated histological findings of lung injury by inhibiting the expression of IL-1β, TNF-α, and IL-6[126]. Birnbaum et al. reported that saxagliptin-mediated DPP4 inhibition could attenuate diabetes mellitus (DM) -induced activation of nod-like receptor family pyrin domain-containing 3 (NLRP3) inflammatory bodies, thus reducing serum CRP, TNF-α, IL-1β, IL-18 and IL-6 levels [127]. CD26 inhibitors, including sitagliptin, alogliptin, vildagliptin, saxagliptin, and linagliptin, are a class of drugs used effectively in the treatment of type 2 diabetes, which has demonstrated safety in elderly patients. These drugs have similar effects by binding to essentially the same catalytic site [128]. Research has shown that the administration of linagliptin can lead to a decrease in the concentration of proinflammatory factors, especially TNF-α and IL-6 [66]. Moreover, mathematical modeling has shown that the spread of MERS-CoV infection can be controlled by inhibiting the expression of CD26, with similar efficiency in SARS-CoV-2 infection [129]. Since the expression of CD26 is closely related to the pathogenesis and severity of COVID-19, CD26 inhibitors have recently been proposed as potential drugsagainst COVID-19 [130]. However, despite laboratory verification and theoretical feasibility, the actual efficacies of CD26 inhibitors in COVID-19 still require verification in further clinical trials. ...
Effective treatment of severe COVID-19 patients with tocilizumab
2
2020
... As we mentioned above, COVID-19 severity and outcomes are closely related to the characteristics of the immuneresponse and subsequent cytokine storm incited by pathogenic T cells and inflammatory monocytes with a high level of IL-6 secretion, which are more severe in elderly patients [131]. Some researchers have recommended monoclonal antibodies that target IL-6,TNF-α and other cytokine pathways as a potential strategy to attenuate the inflammatory storm [132]. ...
... Tocilizumab is a marketed humanized monoclonal antibody that directly targets IL-6 receptors. Accumulating clinical trials have confirmed its safety and effectiveness in rheumatoid arthritis treatment. In a clinical trial among 45 patients, tocilizumab exerted a rapidly beneficial effect on fever and inflammatory markers in COVID-19 patients [133]. According to Xu et al., within 5 days after additional application of tocilizumab, the percentage of lymphocytes in peripheral blood returned to normal in 52.6% of severe COVID-19 patients, and all patients were discharged after anaverage of 15.1 days. The results indicated that tocilizumab could improve the clinical outcomes in severe COVID-19 patients by suppressing the immune response [131]. Recently, tocilizumab was approved for patients with severe SARS-CoV-2 pulmonary complications by the National Health Commission of the People’s Republic of China. Other monoclonal antibodies specifically targeting IL-6 pathways, such as sarilumab and siltuximab, are also recommended for COVID-19 treatment. Clinical trials are still needed to evaluate their efficacy and safety in COVID-19 patients. ...
Anti-IL6R role in treatment of COVID-19-related ARDS
1
2020
... As we mentioned above, COVID-19 severity and outcomes are closely related to the characteristics of the immuneresponse and subsequent cytokine storm incited by pathogenic T cells and inflammatory monocytes with a high level of IL-6 secretion, which are more severe in elderly patients [131]. Some researchers have recommended monoclonal antibodies that target IL-6,TNF-α and other cytokine pathways as a potential strategy to attenuate the inflammatory storm [132]. ...
Off-label use of tocilizumab for the treatment of SARS-CoV-2 pneumonia in Milan, Italy. Eur J
1
2020
... Tocilizumab is a marketed humanized monoclonal antibody that directly targets IL-6 receptors. Accumulating clinical trials have confirmed its safety and effectiveness in rheumatoid arthritis treatment. In a clinical trial among 45 patients, tocilizumab exerted a rapidly beneficial effect on fever and inflammatory markers in COVID-19 patients [133]. According to Xu et al., within 5 days after additional application of tocilizumab, the percentage of lymphocytes in peripheral blood returned to normal in 52.6% of severe COVID-19 patients, and all patients were discharged after anaverage of 15.1 days. The results indicated that tocilizumab could improve the clinical outcomes in severe COVID-19 patients by suppressing the immune response [131]. Recently, tocilizumab was approved for patients with severe SARS-CoV-2 pulmonary complications by the National Health Commission of the People’s Republic of China. Other monoclonal antibodies specifically targeting IL-6 pathways, such as sarilumab and siltuximab, are also recommended for COVID-19 treatment. Clinical trials are still needed to evaluate their efficacy and safety in COVID-19 patients. ...
Immunomodulatory therapy for the management of severe COVID-19. Beyond the anti-viral therapy: A comprehensive review
1
2020
... The cyclosporine-cyclophilin A complex, including cyclophilin and tacrolimus, is considered to suppress organ rejection by halting the expression of TNF-α and IL-2 [134]. Moreover, according to Pfefferle et al., cyclophilin can block the replication of coronaviruses, including SARS-CoV, human CoV-229E and CoV-NL-63, feline CoV, among others. These results suggest that cyclophilin is a broad-spectrum coronavirus inhibitor and might be used for therapy in emerging coronavirus infections [135]. Therefore, the anti-inflammatory and antiviral properties of the cyclosporine-cyclophilin A complex make it a potential clinical application in severe COVID-19. However, considering the nephrotoxicity and hepatotoxicity of cyclophilin and tacrolimus, safety issues must be explored in COVID-19 patients, especially elderly individuals with liver and kidney involvement. ...
The SARS-coronavirus-host interactome: identification of cyclophilins as target for pan-coronavirus inhibitors
1
2011
... The cyclosporine-cyclophilin A complex, including cyclophilin and tacrolimus, is considered to suppress organ rejection by halting the expression of TNF-α and IL-2 [134]. Moreover, according to Pfefferle et al., cyclophilin can block the replication of coronaviruses, including SARS-CoV, human CoV-229E and CoV-NL-63, feline CoV, among others. These results suggest that cyclophilin is a broad-spectrum coronavirus inhibitor and might be used for therapy in emerging coronavirus infections [135]. Therefore, the anti-inflammatory and antiviral properties of the cyclosporine-cyclophilin A complex make it a potential clinical application in severe COVID-19. However, considering the nephrotoxicity and hepatotoxicity of cyclophilin and tacrolimus, safety issues must be explored in COVID-19 patients, especially elderly individuals with liver and kidney involvement. ...
Therapeutic Mechanisms of Glucocorticoids
1
2018
... Corticosteroids show inhibitory effects on both innate and adaptive immune responses, as well as multiple types of immune cells [136]. Corticosteroids were among the first therapies tested in trials for preventing ARDS [137]. Meduri et al. constructed a clinical trial to investigate the efficacy of long-term corticosteroid treatment in patients with ARDS. The results showed that prolonged corticosteroid application could accelerate the resolution of ARDS and decrease hospital mortality [138]. Fadel et al. conducted a single pretest, single posttest quasi-experiment among 213 COVID-19 patients. The results indicated that an early short course of methylprednisolone application could reduce escalation of care and improve clinical outcomes in patients with moderate-to-severe COVID-19 [139]. However, clinical management of severe SARS and MERS patients revealed that corticosteroid therapy did not decrease mortality; in contrast, it caused delayed viral shedding [140]. In addition, Zha et al. announced that after analyzing the data of 31 COVID-19 patients, they found no association between corticosteroid therapy and outcomes in patients without ARDS [141]. The efficacy of corticosteroids in COVID-19 patients remains controversial. Thus, the Guideline for the Diagnosis and Treatment of COVID-19 (7th version) recommended low-to-moderate doses and short courses of corticosteroid application in selected COVID-19 cases that represent excessive immune response activation or rapid progression of imaging changes ...
Ineffectiveness of high-dose methylprednisolone in preventing parenchymal lung injury and improving mortality in patients with septic shock
1
1988
... Corticosteroids show inhibitory effects on both innate and adaptive immune responses, as well as multiple types of immune cells [136]. Corticosteroids were among the first therapies tested in trials for preventing ARDS [137]. Meduri et al. constructed a clinical trial to investigate the efficacy of long-term corticosteroid treatment in patients with ARDS. The results showed that prolonged corticosteroid application could accelerate the resolution of ARDS and decrease hospital mortality [138]. Fadel et al. conducted a single pretest, single posttest quasi-experiment among 213 COVID-19 patients. The results indicated that an early short course of methylprednisolone application could reduce escalation of care and improve clinical outcomes in patients with moderate-to-severe COVID-19 [139]. However, clinical management of severe SARS and MERS patients revealed that corticosteroid therapy did not decrease mortality; in contrast, it caused delayed viral shedding [140]. In addition, Zha et al. announced that after analyzing the data of 31 COVID-19 patients, they found no association between corticosteroid therapy and outcomes in patients without ARDS [141]. The efficacy of corticosteroids in COVID-19 patients remains controversial. Thus, the Guideline for the Diagnosis and Treatment of COVID-19 (7th version) recommended low-to-moderate doses and short courses of corticosteroid application in selected COVID-19 cases that represent excessive immune response activation or rapid progression of imaging changes ...
Prolonged Glucocorticoid Treatment in ARDS: Impact on Intensive Care Unit-Acquired Weakness
1
2016
... Corticosteroids show inhibitory effects on both innate and adaptive immune responses, as well as multiple types of immune cells [136]. Corticosteroids were among the first therapies tested in trials for preventing ARDS [137]. Meduri et al. constructed a clinical trial to investigate the efficacy of long-term corticosteroid treatment in patients with ARDS. The results showed that prolonged corticosteroid application could accelerate the resolution of ARDS and decrease hospital mortality [138]. Fadel et al. conducted a single pretest, single posttest quasi-experiment among 213 COVID-19 patients. The results indicated that an early short course of methylprednisolone application could reduce escalation of care and improve clinical outcomes in patients with moderate-to-severe COVID-19 [139]. However, clinical management of severe SARS and MERS patients revealed that corticosteroid therapy did not decrease mortality; in contrast, it caused delayed viral shedding [140]. In addition, Zha et al. announced that after analyzing the data of 31 COVID-19 patients, they found no association between corticosteroid therapy and outcomes in patients without ARDS [141]. The efficacy of corticosteroids in COVID-19 patients remains controversial. Thus, the Guideline for the Diagnosis and Treatment of COVID-19 (7th version) recommended low-to-moderate doses and short courses of corticosteroid application in selected COVID-19 cases that represent excessive immune response activation or rapid progression of imaging changes ...
Early Short Course Corticosteroids in Hospitalized Patients with COVID-19
1
2020
... Corticosteroids show inhibitory effects on both innate and adaptive immune responses, as well as multiple types of immune cells [136]. Corticosteroids were among the first therapies tested in trials for preventing ARDS [137]. Meduri et al. constructed a clinical trial to investigate the efficacy of long-term corticosteroid treatment in patients with ARDS. The results showed that prolonged corticosteroid application could accelerate the resolution of ARDS and decrease hospital mortality [138]. Fadel et al. conducted a single pretest, single posttest quasi-experiment among 213 COVID-19 patients. The results indicated that an early short course of methylprednisolone application could reduce escalation of care and improve clinical outcomes in patients with moderate-to-severe COVID-19 [139]. However, clinical management of severe SARS and MERS patients revealed that corticosteroid therapy did not decrease mortality; in contrast, it caused delayed viral shedding [140]. In addition, Zha et al. announced that after analyzing the data of 31 COVID-19 patients, they found no association between corticosteroid therapy and outcomes in patients without ARDS [141]. The efficacy of corticosteroids in COVID-19 patients remains controversial. Thus, the Guideline for the Diagnosis and Treatment of COVID-19 (7th version) recommended low-to-moderate doses and short courses of corticosteroid application in selected COVID-19 cases that represent excessive immune response activation or rapid progression of imaging changes ...
SARS: systematic review of treatment effects
1
2006
... Corticosteroids show inhibitory effects on both innate and adaptive immune responses, as well as multiple types of immune cells [136]. Corticosteroids were among the first therapies tested in trials for preventing ARDS [137]. Meduri et al. constructed a clinical trial to investigate the efficacy of long-term corticosteroid treatment in patients with ARDS. The results showed that prolonged corticosteroid application could accelerate the resolution of ARDS and decrease hospital mortality [138]. Fadel et al. conducted a single pretest, single posttest quasi-experiment among 213 COVID-19 patients. The results indicated that an early short course of methylprednisolone application could reduce escalation of care and improve clinical outcomes in patients with moderate-to-severe COVID-19 [139]. However, clinical management of severe SARS and MERS patients revealed that corticosteroid therapy did not decrease mortality; in contrast, it caused delayed viral shedding [140]. In addition, Zha et al. announced that after analyzing the data of 31 COVID-19 patients, they found no association between corticosteroid therapy and outcomes in patients without ARDS [141]. The efficacy of corticosteroids in COVID-19 patients remains controversial. Thus, the Guideline for the Diagnosis and Treatment of COVID-19 (7th version) recommended low-to-moderate doses and short courses of corticosteroid application in selected COVID-19 cases that represent excessive immune response activation or rapid progression of imaging changes ...
Corticosteroid treatment of patients with coronavirus disease 2019 (COVID-19)
1
2020
... Corticosteroids show inhibitory effects on both innate and adaptive immune responses, as well as multiple types of immune cells [136]. Corticosteroids were among the first therapies tested in trials for preventing ARDS [137]. Meduri et al. constructed a clinical trial to investigate the efficacy of long-term corticosteroid treatment in patients with ARDS. The results showed that prolonged corticosteroid application could accelerate the resolution of ARDS and decrease hospital mortality [138]. Fadel et al. conducted a single pretest, single posttest quasi-experiment among 213 COVID-19 patients. The results indicated that an early short course of methylprednisolone application could reduce escalation of care and improve clinical outcomes in patients with moderate-to-severe COVID-19 [139]. However, clinical management of severe SARS and MERS patients revealed that corticosteroid therapy did not decrease mortality; in contrast, it caused delayed viral shedding [140]. In addition, Zha et al. announced that after analyzing the data of 31 COVID-19 patients, they found no association between corticosteroid therapy and outcomes in patients without ARDS [141]. The efficacy of corticosteroids in COVID-19 patients remains controversial. Thus, the Guideline for the Diagnosis and Treatment of COVID-19 (7th version) recommended low-to-moderate doses and short courses of corticosteroid application in selected COVID-19 cases that represent excessive immune response activation or rapid progression of imaging changes ...
Mesenchymal Stem Cells - Sources and Clinical Applications
1
2008
... MSCs are nonhematopoietic stem cells derived from the mesoderm, which can be isolated from various tissues, such as bone marrow, adipose tissue, umbilical cord blood, placenta, menstrual blood, dental pulp, and amniotic fluid [142]. Accumulating evidence from preclinical and clinical trials has demonstrated that MSCs have great advantages in anti-inflammation, anti-fibrosis and injury repair [143-145]. Shao et al. reported that MSCs could strongly suppress IL-6 production, thereby disrupting the development of cytokine storms [146]. Previously, it was demonstrated that MSC transplantation could significantly reduce the mortality of patients with H7N9-induced ARDS (17.6% died in the MSC group, whereas54.5% died in the control group). Moreover, no significant adverse effects were observed in these patients [147]. According to Leng et al., MSC transplantation could significantly improve pulmonary function and symptoms of COVID-19 patients without obvious adverse effects. Moreover, decreased TNF-α and increased IL-10 levels were detected in the MSC treatment group compared with the control group [148]. These results indicated that MSC-based therapy could be a potential alternative for managing patients with severe symptoms of COVID-19. ...
Immunosuppressive mechanisms of embryonic stem cells and mesenchymal stem cells in alloimmune response
1
2011
... MSCs are nonhematopoietic stem cells derived from the mesoderm, which can be isolated from various tissues, such as bone marrow, adipose tissue, umbilical cord blood, placenta, menstrual blood, dental pulp, and amniotic fluid [142]. Accumulating evidence from preclinical and clinical trials has demonstrated that MSCs have great advantages in anti-inflammation, anti-fibrosis and injury repair [143-145]. Shao et al. reported that MSCs could strongly suppress IL-6 production, thereby disrupting the development of cytokine storms [146]. Previously, it was demonstrated that MSC transplantation could significantly reduce the mortality of patients with H7N9-induced ARDS (17.6% died in the MSC group, whereas54.5% died in the control group). Moreover, no significant adverse effects were observed in these patients [147]. According to Leng et al., MSC transplantation could significantly improve pulmonary function and symptoms of COVID-19 patients without obvious adverse effects. Moreover, decreased TNF-α and increased IL-10 levels were detected in the MSC treatment group compared with the control group [148]. These results indicated that MSC-based therapy could be a potential alternative for managing patients with severe symptoms of COVID-19. ...
The Role of Mesenchymal Stem Cells in Radiation-Induced Lung Fibrosis
0
2019
Activation of p70S6 Kinase-1 in Mesenchymal Stem Cells Is Essential to Lung Tissue Repair
1
2018
... MSCs are nonhematopoietic stem cells derived from the mesoderm, which can be isolated from various tissues, such as bone marrow, adipose tissue, umbilical cord blood, placenta, menstrual blood, dental pulp, and amniotic fluid [142]. Accumulating evidence from preclinical and clinical trials has demonstrated that MSCs have great advantages in anti-inflammation, anti-fibrosis and injury repair [143-145]. Shao et al. reported that MSCs could strongly suppress IL-6 production, thereby disrupting the development of cytokine storms [146]. Previously, it was demonstrated that MSC transplantation could significantly reduce the mortality of patients with H7N9-induced ARDS (17.6% died in the MSC group, whereas54.5% died in the control group). Moreover, no significant adverse effects were observed in these patients [147]. According to Leng et al., MSC transplantation could significantly improve pulmonary function and symptoms of COVID-19 patients without obvious adverse effects. Moreover, decreased TNF-α and increased IL-10 levels were detected in the MSC treatment group compared with the control group [148]. These results indicated that MSC-based therapy could be a potential alternative for managing patients with severe symptoms of COVID-19. ...
Exosomes derived from human umbilical cord mesenchymal stem cells ameliorate IL-6-induced acute liver injury through miR-455-3p
1
2020
... MSCs are nonhematopoietic stem cells derived from the mesoderm, which can be isolated from various tissues, such as bone marrow, adipose tissue, umbilical cord blood, placenta, menstrual blood, dental pulp, and amniotic fluid [142]. Accumulating evidence from preclinical and clinical trials has demonstrated that MSCs have great advantages in anti-inflammation, anti-fibrosis and injury repair [143-145]. Shao et al. reported that MSCs could strongly suppress IL-6 production, thereby disrupting the development of cytokine storms [146]. Previously, it was demonstrated that MSC transplantation could significantly reduce the mortality of patients with H7N9-induced ARDS (17.6% died in the MSC group, whereas54.5% died in the control group). Moreover, no significant adverse effects were observed in these patients [147]. According to Leng et al., MSC transplantation could significantly improve pulmonary function and symptoms of COVID-19 patients without obvious adverse effects. Moreover, decreased TNF-α and increased IL-10 levels were detected in the MSC treatment group compared with the control group [148]. These results indicated that MSC-based therapy could be a potential alternative for managing patients with severe symptoms of COVID-19. ...
Clinical study of mesenchymal stem cell treating acute respiratory distress syndrome induced by epidemic Influenza A (H7N9) infection, a hint for COVID-19 treatment
1
2020
... MSCs are nonhematopoietic stem cells derived from the mesoderm, which can be isolated from various tissues, such as bone marrow, adipose tissue, umbilical cord blood, placenta, menstrual blood, dental pulp, and amniotic fluid [142]. Accumulating evidence from preclinical and clinical trials has demonstrated that MSCs have great advantages in anti-inflammation, anti-fibrosis and injury repair [143-145]. Shao et al. reported that MSCs could strongly suppress IL-6 production, thereby disrupting the development of cytokine storms [146]. Previously, it was demonstrated that MSC transplantation could significantly reduce the mortality of patients with H7N9-induced ARDS (17.6% died in the MSC group, whereas54.5% died in the control group). Moreover, no significant adverse effects were observed in these patients [147]. According to Leng et al., MSC transplantation could significantly improve pulmonary function and symptoms of COVID-19 patients without obvious adverse effects. Moreover, decreased TNF-α and increased IL-10 levels were detected in the MSC treatment group compared with the control group [148]. These results indicated that MSC-based therapy could be a potential alternative for managing patients with severe symptoms of COVID-19. ...
Transplantation of ACE2(-) Mesenchymal Stem Cells Improves the Outcome of Patients with COVID-19 Pneumonia
1
2020
... MSCs are nonhematopoietic stem cells derived from the mesoderm, which can be isolated from various tissues, such as bone marrow, adipose tissue, umbilical cord blood, placenta, menstrual blood, dental pulp, and amniotic fluid [142]. Accumulating evidence from preclinical and clinical trials has demonstrated that MSCs have great advantages in anti-inflammation, anti-fibrosis and injury repair [143-145]. Shao et al. reported that MSCs could strongly suppress IL-6 production, thereby disrupting the development of cytokine storms [146]. Previously, it was demonstrated that MSC transplantation could significantly reduce the mortality of patients with H7N9-induced ARDS (17.6% died in the MSC group, whereas54.5% died in the control group). Moreover, no significant adverse effects were observed in these patients [147]. According to Leng et al., MSC transplantation could significantly improve pulmonary function and symptoms of COVID-19 patients without obvious adverse effects. Moreover, decreased TNF-α and increased IL-10 levels were detected in the MSC treatment group compared with the control group [148]. These results indicated that MSC-based therapy could be a potential alternative for managing patients with severe symptoms of COVID-19. ...
Artificial extracorporeal liver support therapy in patients with severe liver failure
1
2011
... The artificial liver system (ALS) is widely used as an effective support therapy in severe liver failure patients [149]. As mentioned above, the cytokine storm is the main motivator of COVID-19 progression and a poor prognosis, and its severity is closely associated with advanced age. Previously, clinical trials have demonstrated that the plasma exchange module of ALS exhibited high efficacy in attenuating the cytokine storm of H7N9 infection [150]. A single-center study showed that artificial liver plasma exchange could significantly reduce inflammatory cytokine levels, thus reducing mortality in critically ill patients with COVID-19 [151]. Our colleagues found that the application of ALS showed excellent prognosis in the treatment of severeCOVID-19 patients presenting a cytokine storm [152]. According to the Diagnosis and Treatment of COVID-19 (7th version) published in China, ALS is recommended in patients who exhibit rapid disease progression confirmed by lung imaging and a cytokine storm. ...
Evaluation of plasma exchange and continuous veno-venous hemofiltration for the treatment of severe avian influenza A (H7N9): a cohort study
1
2015
... The artificial liver system (ALS) is widely used as an effective support therapy in severe liver failure patients [149]. As mentioned above, the cytokine storm is the main motivator of COVID-19 progression and a poor prognosis, and its severity is closely associated with advanced age. Previously, clinical trials have demonstrated that the plasma exchange module of ALS exhibited high efficacy in attenuating the cytokine storm of H7N9 infection [150]. A single-center study showed that artificial liver plasma exchange could significantly reduce inflammatory cytokine levels, thus reducing mortality in critically ill patients with COVID-19 [151]. Our colleagues found that the application of ALS showed excellent prognosis in the treatment of severeCOVID-19 patients presenting a cytokine storm [152]. According to the Diagnosis and Treatment of COVID-19 (7th version) published in China, ALS is recommended in patients who exhibit rapid disease progression confirmed by lung imaging and a cytokine storm. ...
Critically ill patients with COVID-19 with ECMO and artificial liver plasma exchange: A retrospective study
1
2020
... The artificial liver system (ALS) is widely used as an effective support therapy in severe liver failure patients [149]. As mentioned above, the cytokine storm is the main motivator of COVID-19 progression and a poor prognosis, and its severity is closely associated with advanced age. Previously, clinical trials have demonstrated that the plasma exchange module of ALS exhibited high efficacy in attenuating the cytokine storm of H7N9 infection [150]. A single-center study showed that artificial liver plasma exchange could significantly reduce inflammatory cytokine levels, thus reducing mortality in critically ill patients with COVID-19 [151]. Our colleagues found that the application of ALS showed excellent prognosis in the treatment of severeCOVID-19 patients presenting a cytokine storm [152]. According to the Diagnosis and Treatment of COVID-19 (7th version) published in China, ALS is recommended in patients who exhibit rapid disease progression confirmed by lung imaging and a cytokine storm. ...
A Promising Anti-Cytokine-Storm Targeted Therapy for COVID-19: The Artificial-Liver Blood-Purification System
1
2020
... The artificial liver system (ALS) is widely used as an effective support therapy in severe liver failure patients [149]. As mentioned above, the cytokine storm is the main motivator of COVID-19 progression and a poor prognosis, and its severity is closely associated with advanced age. Previously, clinical trials have demonstrated that the plasma exchange module of ALS exhibited high efficacy in attenuating the cytokine storm of H7N9 infection [150]. A single-center study showed that artificial liver plasma exchange could significantly reduce inflammatory cytokine levels, thus reducing mortality in critically ill patients with COVID-19 [151]. Our colleagues found that the application of ALS showed excellent prognosis in the treatment of severeCOVID-19 patients presenting a cytokine storm [152]. According to the Diagnosis and Treatment of COVID-19 (7th version) published in China, ALS is recommended in patients who exhibit rapid disease progression confirmed by lung imaging and a cytokine storm. ...
COVID-19: The Inflammation Link and the Role of Nutrition in Potential Mitigation
2
2020
... To date, considerable evidence has demonstrated that food and nutrients could affect immune system function. Poor nutritional status is widely considered one of the significant risk factors for severe COVID-19 [153]. It has been directly highlighted that nutritional support may play an important role in determining COVID-19 outcomes [154]. Generally, there are nutritional deficiencies in calcium, vitamin C, vitamin D, folate, and zinc among the elderly population, especially among in-hospital patients [155]. According to a study in Wuhan, the prevalence of malnutrition is elevated in elderly patients with COVID-19 [156]. The researchers suggested that nutritional support should be strengthened during treatment. Malnutrition can exacerbate the immune system deficiency in elderly individuals, making them susceptible to SARS-CoV-2 infection [157]. A healthy, balanced diet can provide elderly individuals with necessary macro- and micronutrients, prebiotics, probiotics, and symbiotics to restore and maintain immune cell function, thus reducing the incidence of SARS-CoV-2 infection [153]. ...
... ]. A healthy, balanced diet can provide elderly individuals with necessary macro- and micronutrients, prebiotics, probiotics, and symbiotics to restore and maintain immune cell function, thus reducing the incidence of SARS-CoV-2 infection [153]. ...
Nutrition support in the time of SARS-CoV-2 (COVID-19)
1
2020
... To date, considerable evidence has demonstrated that food and nutrients could affect immune system function. Poor nutritional status is widely considered one of the significant risk factors for severe COVID-19 [153]. It has been directly highlighted that nutritional support may play an important role in determining COVID-19 outcomes [154]. Generally, there are nutritional deficiencies in calcium, vitamin C, vitamin D, folate, and zinc among the elderly population, especially among in-hospital patients [155]. According to a study in Wuhan, the prevalence of malnutrition is elevated in elderly patients with COVID-19 [156]. The researchers suggested that nutritional support should be strengthened during treatment. Malnutrition can exacerbate the immune system deficiency in elderly individuals, making them susceptible to SARS-CoV-2 infection [157]. A healthy, balanced diet can provide elderly individuals with necessary macro- and micronutrients, prebiotics, probiotics, and symbiotics to restore and maintain immune cell function, thus reducing the incidence of SARS-CoV-2 infection [153]. ...
Food and nutrient intake of Irish community-dwelling elderly subjects: who is at nutritional risk?
1
2014
... To date, considerable evidence has demonstrated that food and nutrients could affect immune system function. Poor nutritional status is widely considered one of the significant risk factors for severe COVID-19 [153]. It has been directly highlighted that nutritional support may play an important role in determining COVID-19 outcomes [154]. Generally, there are nutritional deficiencies in calcium, vitamin C, vitamin D, folate, and zinc among the elderly population, especially among in-hospital patients [155]. According to a study in Wuhan, the prevalence of malnutrition is elevated in elderly patients with COVID-19 [156]. The researchers suggested that nutritional support should be strengthened during treatment. Malnutrition can exacerbate the immune system deficiency in elderly individuals, making them susceptible to SARS-CoV-2 infection [157]. A healthy, balanced diet can provide elderly individuals with necessary macro- and micronutrients, prebiotics, probiotics, and symbiotics to restore and maintain immune cell function, thus reducing the incidence of SARS-CoV-2 infection [153]. ...
Prevalence of malnutrition and analysis of related factors in elderly patients with COVID-19 in Wuhan, China
1
2020
... To date, considerable evidence has demonstrated that food and nutrients could affect immune system function. Poor nutritional status is widely considered one of the significant risk factors for severe COVID-19 [153]. It has been directly highlighted that nutritional support may play an important role in determining COVID-19 outcomes [154]. Generally, there are nutritional deficiencies in calcium, vitamin C, vitamin D, folate, and zinc among the elderly population, especially among in-hospital patients [155]. According to a study in Wuhan, the prevalence of malnutrition is elevated in elderly patients with COVID-19 [156]. The researchers suggested that nutritional support should be strengthened during treatment. Malnutrition can exacerbate the immune system deficiency in elderly individuals, making them susceptible to SARS-CoV-2 infection [157]. A healthy, balanced diet can provide elderly individuals with necessary macro- and micronutrients, prebiotics, probiotics, and symbiotics to restore and maintain immune cell function, thus reducing the incidence of SARS-CoV-2 infection [153]. ...
The immune system and the impact of zinc during aging
1
2009
... To date, considerable evidence has demonstrated that food and nutrients could affect immune system function. Poor nutritional status is widely considered one of the significant risk factors for severe COVID-19 [153]. It has been directly highlighted that nutritional support may play an important role in determining COVID-19 outcomes [154]. Generally, there are nutritional deficiencies in calcium, vitamin C, vitamin D, folate, and zinc among the elderly population, especially among in-hospital patients [155]. According to a study in Wuhan, the prevalence of malnutrition is elevated in elderly patients with COVID-19 [156]. The researchers suggested that nutritional support should be strengthened during treatment. Malnutrition can exacerbate the immune system deficiency in elderly individuals, making them susceptible to SARS-CoV-2 infection [157]. A healthy, balanced diet can provide elderly individuals with necessary macro- and micronutrients, prebiotics, probiotics, and symbiotics to restore and maintain immune cell function, thus reducing the incidence of SARS-CoV-2 infection [153]. ...
Safety, tolerability, and immunogenicity of a recombinant adenovirus type-5 vectored COVID-19 vaccine: a dose-escalation, open-label, non-randomised, first-in-human trial
1
2020
... The development of a safe and effective vaccine against SARS-CoV-2 for nonimmune individuals is an urgent and critical task for controlling the ongoing pandemic [68]. The developing coronavirus vaccines and drugs mainly target the spike glycoprotein or S protein, the major inducers of neutralizing antibodies. To date, Wei Chen et al. conducted a dose-escalation, single-center, open-label, nonrandomized, first-in-human trial of a recombinant adenovirus type5-vectored COVID-19 vaccine in Wuhan, China. The vaccine was tolerable and immunogenic 28 days after vaccination. The humoral responses against SARS-CoV-2 peaked at day 28 after vaccination in healthy adults, and rapid specific T-cell responses were noted from day 14 after vaccination [158]. ...
Detection and control of influenza outbreaks in well-vaccinated nursing home populations
1
2004
... However, even if a successful vaccine for SARS-CoV-2 becomes available, an individual’s immune response must be sufficiently strong to respond to the vaccine, and once exposure occurs, the reaction can later confer protection against the pathogen. Thus, vaccines cannot provide complete protection in elderly populations due to age-related declines in immune function and the accumulation of various diseases. According to Montoet al., influenza outbreaks still occur in elderly nursing homes even when vaccination rates reach 80-98% utilization [159]. Thus, the deficiency of the elderly group could become a gap in herd immunity that relies on vaccines. Some researchers recommended remodeling of the senescent immune system of elderly persons by allo-priming as a method to restore cellular immune function. Heterologous immunity can enhance the panviral protection upon each viral exposure, thereby providing long-term protection. The alloantigen priming strategy has been proposed in conjunction with viral-specific vaccines in the elderly population [160]. However, the efficiency requires further exploration. ...
Immunosenescence in aging: between immune cells depletion and cytokines up-regulation
1
2017
... However, even if a successful vaccine for SARS-CoV-2 becomes available, an individual’s immune response must be sufficiently strong to respond to the vaccine, and once exposure occurs, the reaction can later confer protection against the pathogen. Thus, vaccines cannot provide complete protection in elderly populations due to age-related declines in immune function and the accumulation of various diseases. According to Montoet al., influenza outbreaks still occur in elderly nursing homes even when vaccination rates reach 80-98% utilization [159]. Thus, the deficiency of the elderly group could become a gap in herd immunity that relies on vaccines. Some researchers recommended remodeling of the senescent immune system of elderly persons by allo-priming as a method to restore cellular immune function. Heterologous immunity can enhance the panviral protection upon each viral exposure, thereby providing long-term protection. The alloantigen priming strategy has been proposed in conjunction with viral-specific vaccines in the elderly population [160]. However, the efficiency requires further exploration. ...
What's the way out? Potential exit strategies from the COVID-19 lockdown
1
2020
... Moreover, accumulating reports worldwide of some COVID-19 patients testing positive again after initially testing negative indicate the potential of re-infections and short-lasting immunity against COVID-19 [161]. To et al. firstly reported the case of COVID-19 re-infection by a phylogenetically distinct SARS-corona-virus-2 strain [162]. According to Ibarrondo et al., antibody loss in COVID-19 patients is quicker than that reported for SARS-CoV [163]. It means that humoral immunity against SARS-CoV-2 may not be long lasting in human bodies. Consequently, people doubt whether the vaccine could produce long-term immunity in the population. ...
COVID-19 re-infection by a phylogenetically distinct SARS-coronavirus-2 strain confirmed by whole genome sequencing
1
2020
... Moreover, accumulating reports worldwide of some COVID-19 patients testing positive again after initially testing negative indicate the potential of re-infections and short-lasting immunity against COVID-19 [161]. To et al. firstly reported the case of COVID-19 re-infection by a phylogenetically distinct SARS-corona-virus-2 strain [162]. According to Ibarrondo et al., antibody loss in COVID-19 patients is quicker than that reported for SARS-CoV [163]. It means that humoral immunity against SARS-CoV-2 may not be long lasting in human bodies. Consequently, people doubt whether the vaccine could produce long-term immunity in the population. ...
Rapid Decay of Anti-SARS-CoV-2 Antibodies in Persons with Mild Covid-19
1
2020
... Moreover, accumulating reports worldwide of some COVID-19 patients testing positive again after initially testing negative indicate the potential of re-infections and short-lasting immunity against COVID-19 [161]. To et al. firstly reported the case of COVID-19 re-infection by a phylogenetically distinct SARS-corona-virus-2 strain [162]. According to Ibarrondo et al., antibody loss in COVID-19 patients is quicker than that reported for SARS-CoV [163]. It means that humoral immunity against SARS-CoV-2 may not be long lasting in human bodies. Consequently, people doubt whether the vaccine could produce long-term immunity in the population. ...
Bearing the brunt of covid-19: older people in low and middle income countries
1
2020
... The COVID-19 pandemic suggests that we are facing a historic challenge to our capacity to protect the health of our elderly population. Protecting aging populations is now a central question in maintaining global health and biosecurity [4]. Lloyd-Sherlock et al. announced that due to great barriers in access to health services and support, older people in low-and middle-income countries are bearing the brunt of COVID-19 [164]. An open letter suggested that the WHO should act immediately to redress its neglect of older people, and member states must prioritize the needs of the elderly population in national responses and support for low- and middle-income countries [165]. The current results of biomedical, clinical and public health studies also highlight the need for therapy and prevention strategies for aging COVID-19 patients. We hope that this review can provide insight regarding the prevention and treatment of COVID-19 in elderly populations. ...
WHO must prioritise the needs of older people in its response to the covid-19 pandemic
1
2020
... The COVID-19 pandemic suggests that we are facing a historic challenge to our capacity to protect the health of our elderly population. Protecting aging populations is now a central question in maintaining global health and biosecurity [4]. Lloyd-Sherlock et al. announced that due to great barriers in access to health services and support, older people in low-and middle-income countries are bearing the brunt of COVID-19 [164]. An open letter suggested that the WHO should act immediately to redress its neglect of older people, and member states must prioritize the needs of the elderly population in national responses and support for low- and middle-income countries [165]. The current results of biomedical, clinical and public health studies also highlight the need for therapy and prevention strategies for aging COVID-19 patients. We hope that this review can provide insight regarding the prevention and treatment of COVID-19 in elderly populations. ...
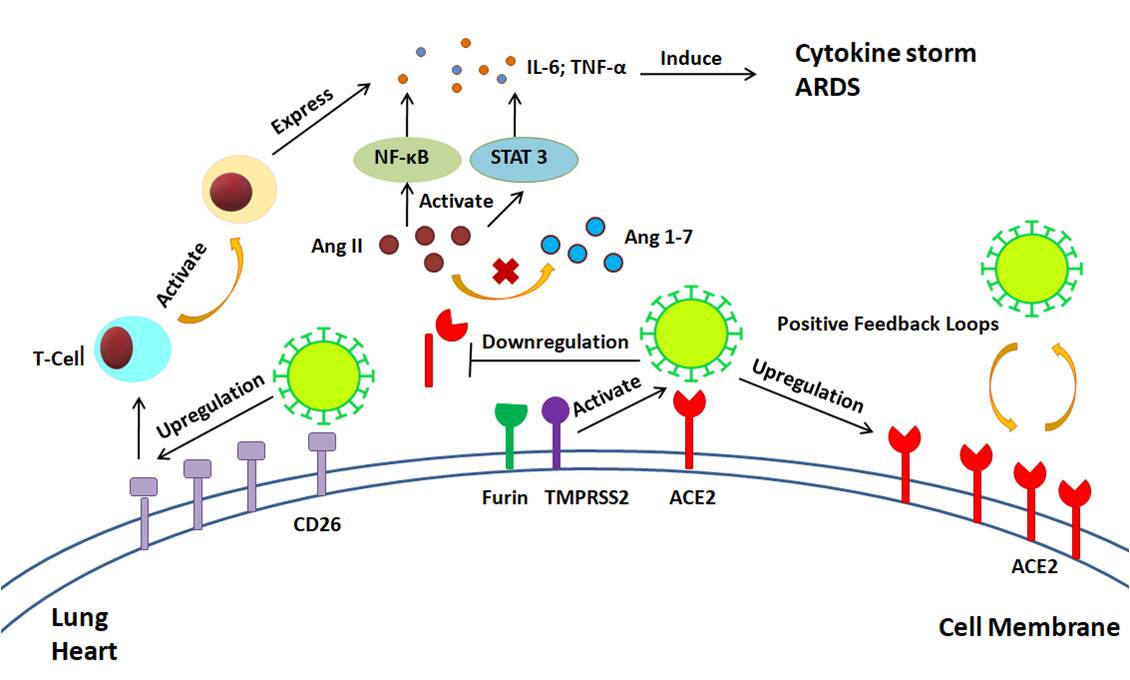
{kind=link}
{kind=link}



