Multi-organ Dysfunction in Patients with COVID-19: A Systematic Review and Meta-analysis
Wu Ting1, 2, Zuo Zhihong1, 3, Kang Shuntong1, 3, Jiang Liping3, Luo Xuan4, Xia Zanxian5, 6, Liu Jing1, Xiao Xiaojuan1, Ye Mao7, Deng Meichun1, 3, 6, *
1Department of Biochemistry and Molecular Biology & Hunan Province Key Laboratory of Basic and Applied Hematology, School of Life Sciences, Central South University, Hunan 410013, China.2Department of Cardiovascular Medicine, The Third Xiangya Hospital, Central South University, Changsha, Hunan 410013, China.3Xiangya School of Medicine, Central South University, Hunan 410013, China.4Hunan Yuanpin Cell Biotechnology Co., Ltd, Hunan 410129, China.5Department of Cell Biology, School of Life Sciences, Central South University, Changsha 410013, China.6Hunan Key Laboratory of Animal Models for Human Diseases, Hunan Key Laboratory of Medical Genetics & Center for Medical Genetics, School of Life Sciences, Central South University, Changsha 410013, China.7Molecular Science and Biomedicine Laboratory, State Key Laboratory for Chemo/Biosensing and Chemometrics, College of Biology, College of Chemistry and Chemical Engineering, Collaborative Innovation Center for Molecular Engineering for Theranostics, Hunan University, Changsha, China
通讯作者: Correspondence should be addressed to: Dr. Meichun Deng, School of Life Sciences, Central South University, Changsha, Hunan, 410013, China. Email: dengmch@csu.edu.cn.Correspondence should be addressed to: Dr. Meichun Deng, School of Life Sciences, Central South University, Changsha, Hunan, 410013, China. Email: dengmch@csu.edu.cn.
收稿日期:2020-05-1
修回日期: 2020-05-18
接受日期: 2020-05-20
网络出版日期: 2020-05-13
版权声明:
2020 This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium provided that the original work is properly attributed.
展开
Abstract
This study aimed to provide systematic evidence for the association between multiorgan dysfunction and COVID-19 development. Several online databases were searched for articles published until May 13, 2020. Two investigators independently selected trials, extracted data, and evaluated the quality of individual trials. Single-arm meta-analysis was performed to summarize the clinical features of confirmed COVID-19 patients. Fixed effects meta-analysis was performed for clinically relevant parameters that were closely related to the patients’ various organ functions. A total of 73 studies, including 171,108 patients, were included in this analysis. The overall incidence of severe COVID-19 and mortality were 24% (95% confidence interval [CI], 20%-28%) and 2% (95% CI, 1%-3%), respectively. Patients with hypertension (odds ratio [OR] = 2.40; 95% CI, 2.08-2.78), cardiovascular disease (CVD) (OR = 3.54; 95% CI, 2.68-4.68), chronic obstructive pulmonary disease (COPD) (OR=3.70; 95% CI, 2.93-4.68), chronic liver disease (CLD) (OR=1.48; 95% CI, 1.09-2.01), chronic kidney disease (CKD) (OR = 1.84; 95% CI, 1.47-2.30), chronic cerebrovascular diseases (OR = 2.53; 95% CI, 1.84-3.49) and chronic gastrointestinal (GI) disease (OR = 2.13; 95% CI, 1.12-4.05) were more likely to develop severe COVID-19. Increased levels of lactate dehydrogenase (LDH), creatine kinase (CK), high-sensitivity cardiac troponin I (hs-cTnI), myoglobin, creatinine, urea, alanine aminotransferase (ALT), aspartate aminotransferase (AST), and total bilirubin were highly associated with severe COVID-19. The incidence of acute organ injuries, including acute cardiac injury (ACI); (OR = 11.87; 95% CI, 7.64-18.46), acute kidney injury (AKI); (OR=10.25; 95% CI, 7.60-13.84), acute respiratory distress syndrome (ARDS); (OR=27.66; 95% CI, 18.58-41.18), and acute cerebrovascular diseases (OR=9.22; 95% CI, 1.61-52.72) was more common in patients with severe COVID-19 than in patients with non-severe COVID-19. Patients with a history of organ dysfunction are more susceptible to severe conditions. COVID-19 can aggravate an acute multiorgan injury.
WuTing, ZuoZhihong, KangShuntong, JiangLiping, LuoXuan, XiaZanxian, LiuJing, XiaoXiaojuan, YeMao, DengMeichun. Multi-organ Dysfunction in Patients with COVID-19: A Systematic Review and Meta-analysis[J]. Aging and Disease, 2020, 11(4): 874-894 https://doi.org/10.14336/AD.2020.0520
Coronaviruses are positive-stranded ribonucleic acid (+RNA) viruses belonging to the family Coronaviridae and order Nidovirales [1, 2]. Prior to December 2019, six coronavirus species had been identified and these primarily caused mild illness [2, 3]. However, in the past decades, two zoonotic coronaviruses, severe acute respiratory syndrome coronavirus (SARS-CoV) and Middle East respiratory syndrome coronavirus (MERS-CoV), resulted in severe and even fatal lower respiratory tract infections, with more than 8000 and 1500 confirmed cases and 10% and 37% case fatality rates (CFR), respectively [4, 5]. Although coronavirus infections have a huge effect, strategies to prevent and treat coronavirus infection are limited due to the lack of effective antiviral treatments [6].
At the beginning of December 2019, pneumonia due to an unknown cause was reported in a series of patients. On January 7, 2020, the cause was identified as a novel coronavirus infection. This virus was named SARS-CoV-2 by the World Health Organization (WHO). Similar to SARS-CoV and MERS-CoV, SARS-CoV-2 targets the respiratory tract and the dominant symptoms of COVID-19 at the beginning of the illness are fever, cough, fatigue, or myalgia [7, 8]. Although COVID-19 has a relatively low CFR, it is spreading rampantly, with more than four million confirmed cases, and it has affected the global economy and human health.
Studies have suggested that COVID-19 leads to the development of severe pneumonia, other complications, and even death, especially in high-risk patients [9, 10]. To date, neither a vaccine nor a specific treatment with a confirmed result has been available to patients. Hence, effective methods to improve the outcomes in patients with severe COVID-19 may include the early prevention of SARS-CoV-2 infection in high-risk patients and the early monitoring and intervention regarding the parameters associated with disease severity. It has been reported that patients with diabetes, hypertension, and coronary heart diseases are 2.85, 3.05, and 21.40 times more likely to have a poor prognosis, respectively, than that in patients without these diseases [10]. In addition, elevated alanine aminotransferase (ALT), lactate dehydrogenase (LDH), high-sensitivity cardiac troponin I (hs-cTnI), and urea levels have been reported to be associated with disease severity [11, 12]. The incidence of complications, including acute respiratory distress syndrome (ARDS) and acute cardiac injury (ACI), is higher in patients with severe COVID-19 [8, 10]. These clinically relevant parameters are closely related to various organ functions in patients. Hence, we wanted to know whether patients with a history of organ dysfunction are more susceptible to COVID-19 infection and whether COVID-19 infection aggravates acute damage to various organs. Given the rapid spread of COVID-19 with no specific treatment available, it is urgent to analyze published and high-quality clinical studies to identify guidelines for the management of the patients. This study aimed to provide systematic evidence for the association between multiorgan dysfunction and COVID-19 severity and to compare differences in the indices of organ function among COVID-19, SARS, and MERS. In addition, based on the existing literature, we have provided certain treatment suggestions for patients with dysfunction of various organs.
MATERIALS AND METHODS
This study was registered in PROSPERO, with registration No. CRD42020177984.
Search strategies
Studies published in the EMBASE, PubMed, Web of Science, MedRxiv, and Biorxiv databases before or on May 13, 2020, were searched using the following search terms: “SARS-2-CoV,” “coronavirus,” “COVID19,” “2019-nCoV,” “clinical features,” “clinical characteristics,” “clinical outcomes,” “cardiac diseases,” “renal diseases,” “pulmonary diseases,” “liver diseases,” “neurological disease,” “gastrointestinal (GI) disease,” “nervous system,” and “digestive system,” alone or in combination, without language restriction.
Eligibility criteria
Eligible studies were included in the meta-analysis according to the following criteria: (1) type of participants: patients (≥18 years old) in each study who were diagnosed as having COVID-19 and (2) type of study: all studies that provide information about symptoms, medical history, laboratory results, and outcomes of COVID-19 patients. Studies that enrolled severe disease and non-severe disease groups (or ICU and non-ICU or death and survival) were included to examine the relationship between organ dysfunction and COVID-19 severity. Trials were excluded if any of the following factors were identified: (1) study design: comments, letters, case reports, abstracts, and reviews; (2) type of participants: animals, patients <18 years old, and pregnant women; and (3) insufficient information concerning evaluation rates.
Trial selection
After eliminating duplicates, two independent investigators reviewed the remaining identified trials to confirm that they fulfilled the inclusion criteria. Finally, the reference lists of the included studies were screened to examine other potentially relevant studies. All the disagreements were discussed and solved after rechecking the source data with the third investigator; in all the cases, one person recognized an error.
Data extraction and quality assessment
Two reviewers extracted data independently using a predefined data extraction form. The data extracted included the last name of the first author, publication year, sample size (n), mean age (years), percentage of female patients (%), study design, geographical region, overall cases (n), symptoms, comorbidities, laboratory findings, and complications. The quality assessment forms recommended by the Agency for Healthcare Research and Quality were used for quality assessment of the included trials. We resolved all disagreements through a discussion.
Statistical analyses
The weighted mean difference (WMD) and odds ratio (OR) were used to compare continuous and dichotomous variables, respectively. All the results were reported with 95% confidence intervals (CIs). Median (range) or median (interquartile range [IQR]) will be converted to the form of mean (standard deviation [SD]) [13]. We pooled the effect estimates of the outcomes by using fixed-effect models. A random effect model was used when significant heterogeneity was detected. Heterogeneity was assessed by using the I2 value, and an I2 of >50% was considered significant. The sensitivity analyses were made by excluding one study at a time to observe the change of the effects on the outcomes. Egger’s test, and Begg’s test (P < 0.10) were used to suggest the possible publication bias of outcomes. We performed all statistical analyses with the STATA 12.0 statistical software package (StataCoporation, College Station, Texas, USA).
Selection of included studies and Study Characteristics
A total of 5037 relevant articles were identified by searching several online databases. Figure 1 presents the screening and selection process of the eligible trials. The characteristics of the included trials are listed in Supplementary Table 1. This meta-analysis included 73 studies [8, 11, 12, 14-83]. Among these studies, 54 were from China, 4 from Italy, 3 from The United States, 2 from The United Kingdom, 2 from France, 2 from Spain, and the remaining 6 from other countries. Clinical features of severe and non-severe COVID-19 cases were reported by 48 studies. The results of the quality assessments were presented in Supplementary Table 1.
The results of this meta-analysis revealed that the overall CFR was 2% (95% confidence interval [CI], 1%-3%) and the proportion of patients with severe illness was 24% (95% CI, 20%-28%). The most common comorbidities were hypertension 19% (95% CI, 15%-23%), followed by diabetes 10% (95% CI, 8%-13%) and cardiovascular disease (CVD) 8% (95% CI, 4%-14%). The prevalence of chronic obstructive pulmonary disease (COPD), cerebrovascular disease, chronic liver disease (CLD), chronic kidney disease (CKD), tumor, chronic GI disease and nervous system disease were 2% (95% CI, 2%-3%), 3% (95% CI, 2%-5%), 3% (95% CI, 2%-4%), 3% (95% CI, 1%-4%), 3% (95% CI, 1%-5%), 7% (95% CI, 5%-8%), and 1% (95% CI, 0%-2%), respectively. Furthermore, we analyzed the prevalence of complications caused by COVID-19. The most common complications were ARDS 12% (95% CI, 7%-18%), followed by ACI 6% (95% CI, 3%-9%) and shock 6% (95% CI, 2%-11%). The overall proportion of acute kidney disease (AKI) and acute cerebrovascular disease was 4% (95% CI, 1%-7%) and 2% (95% CI, 1%-3%), respectively. The laboratory results revealed that cardiac function indexes, such as LDH (275.43 U/L; 95% CI, 247.82-303.04 U/L) and myoglobin (49.96 ng/mL; 95% CI, 37.11-62.81. ng/mL) levels were elevated. The pooled results of the included studies showed that the most common neurologic symptoms were olfactory and/or taste disorders (54%; 95% CI, 37%-70%), and the most dominant GI symptom was anorexia (21%; 95% CI, 14%-29%) (Table 1). Notably, olfactory and/or taste disorders were less common in Asia. The pooled results were from the included studies which were outside of Asia.
Figure 2. Relationship between cardiac dysfunction (Hypertension, CVD, CK and LDH) and COVID-19 severity.
Organ dysfunction and COVID-19 severity
Cardiac dysfunction
We analyzed the relationship between cardiac dysfunction and the development of COVID-19. Disease severity was found to be closely associated with the history of hypertension (odds ratio [OR] = 2.40; 95% CI, 2.08-2.78) and CVD (OR = 3.54; 95% CI, 2.68-4.68). Obvious differences in LDH (weighted mean difference [WMD] = 140.27 U/L; 95% CI, 102.18-178.36 U/L), CK (WMD =34.01 U/L; 95% CI, 9.46-58.59 U/L), hs-cTnI (WMD =15.99 pg/mL; 95% CI, 6.24-25.74 pg/mL), and myoglobin (WMD = 41.21 ng/mL; 95% CI, 25.85-56.56. ng/mL) levels were noted between patients with severe and non-severe COVID-19. In addition, a significantly higher incidence of ACI was observed among patients with severe COVID-19 than that among patients with non-severe COVID-19 (OR = 11.87; 95% CI, 7.64-18.46). Patients with severe COVID-19 were more likely to experience arrhythmias (OR = 14.76; 95% CI, 8.87-24.56). In addition, we found preexisting diabetes was positively associated with COVID-19 severity (OR = 2.25; 95% CI, 1.91-2.65) (Fig. 2 and 3 and supplemtary Fig. 1).
Figure 3. Relationship between cardiac dysfunction (hs-cTnI, myoglobin, ACI and arrhythmia) and COVID-19 severity.
Treatment suggestions
In the preclinical in vitro studies, chloroquine (CQ) was found to inhibit SARS-CoV-2 activity [84]. Hydroxychloroquine (HCQ), a derivative of CQ, was found to be more potent than CQ in vitro. In addition, researchers have confirmed the clinical benefits of CQ for SARS [85]. A randomized clinical trial found that HCQ significantly shortened the time to clinical recovery and promoted pneumonia absorption among COVID-19 patients [86]. Therefore, the guidelines recommend that the administration of CQ/HCQ may help to improve the clinical outcomes of COVID-19 patients. However, the efficiency and safety of CQ and HCQ for treating COVID-19 remain uncertain due to recent controversial results [87], especially its’ potential cardiac toxicity. CQ/HCQ alone can cause QT prolongation and is known to cause torsades de pointes, especially among patients with a history of cardiac dysfunction and when administered in combination with other drugs such as lopinavir/ritonavir (LPV/r); [88]. It was reported that 30% of patients treated with HCQ + azithromycin developed new QT prolongation of > 40 ms [89]. Therefore, we strongly recommend close monitoring of electrocardiograms with QTc evaluation and correction of any electrolyte imbalance prior to administering CQ/HCQ [90]. Non-essential QT-prolonging drugs, including LPV/r, should be avoided in patients with a history of cardiac dysfunction.
Renal dysfunction
The pooled results indicated that patients with CKD were at a high risk of developing severe COVID-19 (OR = 1.84; 95% CI, 1.47-2.30). Patients with severe COVID-19 had higher levels of creatinine (WMD = 10.40 μmol/L; 95% CI, 8.07-12.72 μmol/L) and urea (WMD = 1.61 mmol/L; 95% CI, 1.26-1.96mmol/L) than those in patients with non-severe COVID-19. Furthermore, because severe infection aggravates kidney damage, AKI was more likely to occur among patients with severe COVID-19 than among patients with non-severe COVID-19 (OR=10.25; 95% CI, 7.60-13.84) (Fig. 4).
Figure 4. Relationship between renal dysfunction and COVID-19 severity.
Treatment suggestions
The present study revealed that the overall proportion of AKI was 4% (95% CI, 1%-7%) and AKI was associated with in-hospital mortality of COVID-19 patients [91]. According to the latest treatment protocol (Pilot Version 7) issued by the Chinese Health Commission, continuous renal replacement therapy (CRRT) is recommended for patients with severe COVID-19 and renal damage, especially for those with stage 3 AKI. CRRT removes inflammatory cytokines to regulate renal metabolic adaptation and improves kidney energy balance to protect the kidneys in patients with AKI [92]. Wang et al. suggested that COVID-19 patients with renal dysfunction should be monitored regularly. Once acute kidney failure develops, potential interventions, including CRRT, should be immediately initiated to protect renal function [93]. However, CRRT intensity should be carefully determined. A study indicated that higher-intensity CRRT treatment did not reduce mortality in patients with severe COVID-19 and AKI as compared with that in the control group [94].
Pulmonary dysfunction
COPD (OR = 3.70; 95% CI, 2.93-4.68) and smoking (OR = 1.61; 95% CI, 1.28-2.02) were significant predictors of severe COVID-19. Patients who presented with bilateral involvement on chest radiography on admission were four times more likely to develop severe COVID-19 (OR = 4.65; 95% CI, 2.94-7.34). Finally, patients with severe COVID-19 were found to have a significantly higher risk of developing ARDS compared to that in those with non-severe COVID-19 (OR=27.66; 95% CI, 18.58-41.18). (Fig. 5).
Treatment suggestion
Corticosteroid treatment is a double-edged sword and its’ effectiveness in treating COVID-19 remains controversial. One study indicated that delayed viral clearance was not observed in patients treated with low dose corticosteroids, while another trial revealed that patients treated with a corticosteroid demonstrated more abnormalities on chest CT and more clinical symptoms [95, 96]. ARDS, the leading cause of death in patients with SARS and MERS, is also a challenge in COVID-19 patients. ARDS is closely associated with overwhelming inflammation and cytokine-related lung injury. A retrospective cohort study revealed that methylprednisolone treatment appears to reduce the risk of death in COVID-19 patients with ARDS (HR = 0.38; 95% CI, 0.20-0.72) [97]. Given the urgent clinical demand, corticosteroid treatment is weakly recommended for COVID-19 patients with ARDS due to the low-quality evidence. However, it is not recommended for routine treatment [98].
Figure 5. Relationship between pulmonary dysfunction and COVID-19 severity
Liver dysfunction
We analyzed the relationship between liver dysfunction and COVID-19 severity. CLD was a significant predictor of COVID-19 severity (OR = 1.48; 95% CI, 1.09-2.01). Significant differences in ALT (WMD = 7.11 U/L; 95% CI, 5.47-8.75 U/L), aspartate aminotransferase (AST; WMD = 16.10 U/L; 95% CI, 14.00-18.20 U/L), and total bilirubin (WMD = 2.75 mmol/L; 95% CI, 2.11-3.40 mmol/L) were observed in patients with severe and non-severe COVID-19. One study specifically presented a higher incidence of acute liver injury in patients with severe COVID-19 as compared with that in patients with non-severe COVID-19. This is consistent with laboratory indicators [29] (Fig. 6).
Treatment suggestion
One study found that SARS patients treated with LPV/r appeared to have a milder disease course, better outcomes, and significantly reduced viral loads [99]. Similarly, lopinavir has activity against MERS-CoV [100, 101]. As LPV/r is effective against other coronaviruses, researchers were optimistic to prescribe LPV/r for the treatment of COVID-19. However, a randomized, controlled, open-label trial conducted in China revealed that no significant difference was observed between LPV/r treatment and the control group of patients with severe COVID-19 in clinical improvement, reduced mortality, and/or changes in viral load [102]. The liver biopsy results of fatal COVID-19 patients indicated that the possibility of drug-induced acute liver injury could not be ruled out [103]. A study identified that patients with liver damage were administered a higher rate of LPV/r than that in those with normal liver function [104]. Hence, we do not recommend LPV/r as a routine treatment option for patients with a history of liver dysfunction. Further, clinicians should closely monitor liver-function indicators even in patients with normal liver function, if they are being treated with LPV/r.
Figure 6. Relationship between liver dysfunction and COVID-19 severity
Neurologic dysfunction
Patients with chronic cerebrovascular diseases tended to face a higher risk of developing severe COVID-19 compared to those without chronic cerebrovascular diseases (OR = 2.53; 95% CI, 1.84-3.49). Patients with severe COVID-19 were more likely to have nervous system manifestations, such as dizziness (OR = 1.99; 95% CI, 1.23-3.24) and impaired consciousness (OR = 4.52; 95% CI, 2.25-9.06). Few differences in the incidence of headache (OR = 1.17; 95% CI, 0.90-1.52) and olfactory disorders (OR = 0.67; 95% CI, 0.21-2.15) were noted between patients with severe and non-severe COVID-19. Acute cerebrovascular diseases were significantly more common in severe infection compared with non-severe infection (OR = 9.22; 95% CI, 1.61-52.72) (Fig. 7)
Figure 7. Relationship between neurologic dysfunction and COVID-19 severity.
Treatment suggestions
Ischemic stroke has been recognized as a complication in patients with COVID-19, especially in patients with severe infection [105]. However, the precise mechanisms are not yet clear. Obviously, an elevated D-dimer level was noted in patients with COVID-19 who developed stroke, indicating a hypercoagulable state [106]. It was suggested that production of antiphospholipid antibodies (aPL) accompanying COVID-19 infection may be closely associated with both venous and arterial thrombotic events [107]. The mortality of COVID-19 patients with stroke was much higher than that of patients with stroke alone [106, 108]. Considering the high mortality and prothrombotic state, it seems reasonable to initiate treatment with anticoagulants such as low molecular weight heparin (LMWH) and a recombinant tissue plasminogen activator (rt-PA) [109]. Compared with antiplatelet treatment, patients treated with LMWH had lower mortality [106]. Notably, patients who developed stroke were more likely to have multiple organ dysfunction [106]. Patients with hepatic dysfunction may have a significant reduction in their ability of hepatic clearance, which would increase the risk of intracranial hemorrhage (ICH). In addition, leukocytosis, elevated C reactive protein levels and D-dimer, which were commonly seen in COVID-19 patients, were identified as risk factors of ICH among patients without COVID-19 infection [110]. Therefore, it is reasonable to assess the coagulation profile for COVID-19 patients with acute ischemic stroke prior to administration of rt-PA and LMWH to determine the risk benefit ratio [109].
Gastrointestinal dysfunction
Chronic GI diseases were closely associated with severe infection (OR = 2.13; 95% CI, 1.12-4.05). GI symptoms, including nausea and/or vomiting (OR=1.57; 95% CI, 1.08-2.29), anorexia (OR = 3.35; 95% CI, 1.87-6.00) and abdominal pain (OR = 2.63; 95% CI, 1.41-4.90) were more likely to be observed in severe COVID-19 patients compared with non-severe COVID-19 patients. However, the incidence of diarrhea (OR=1.18; 95% CI, 0.95-1.47) and vomiting (OR=1.97; 95% CI, 0.93-4.19) were similar in patients with severe and non-severe COVID-19 (Fig. 8).
Treatment suggestion
As the COVID-19 pandemic expands, the impact of COVID-19 on patients with inflammatory bowel disease (IBD) has been a major concern. A significant number of IBD patients require immunosuppressors that target extensive inflammation. This may weaken the immune system and predispose IBD patients to a higher risk of COVID-19 infection. However, according to evidence emerging from China, Italy and other counties, there was no obvious indication that IBD patients were at greater risk of COVID-19 infection compared to the general population [111-113]. Thiopurines were related to a risk of serious viral infection in IBD patients, while a meta-analysis revealed that anti-tumor necrosis factor therapy was associated developing an opportunistic infection [114, 115]. However, discontinuation of IBD drugs should not be recommended for IBD patients during the COVID-19 pandemic [111]. This was supported by the results of the first case series report of COVID-19 infection in IBD patients [116]. Clinicians should be alert regarding patients treated with immunosuppressors and carefully monitor the presence of symptoms associated with COVID-19 [117]. The withholding of ongoing therapies should be considered only in confirmed COVID-19 patients. Therapies must be assessed carefully according to the balance between the severity of COVID-19 and the status of IBD [118].
Table 2
Table 2 Comparison of impacts of organ function on severity of COVID-19, MERS and SARS.
Figure 8. Relationship between gastrointestinal dysfunction and COVID-19 severity.
Comparison of the impact of organ dysfunction on the severity of COVID-19, MERS, and SARS
We searched related articles to undertake a meta-analysis of SARS and MERS. The strategies were similar to COVID-19 [119-137].
CVD is a risk factor for predicting the severity of COVID-19, MERS, and SARS [138]. Similar to COVID-19 patients, LDH (WMD = 124.14 U/L; 95% CI, 31.09-217.19 U/L) and CK (WMD = 149.91 U/L; 95% CI, 94.03-205.79 U/L) levels of patients with severe SARS are frequently high. However, few studies have compared LDH and CK levels in patients with severe and non-severe MERS. As presented in Table 2, patients with either of the three viruses and renal and pulmonary dysfunction on admission were at high risk of developing severe disease. CLD was also a risk factor for the severity of SARS and MERS. No significant differences in ALT levels (WMD = -3.07 U/L; 95% CI, -11.26-5.11 U/L) or AST levels (WMD = 34.81 U/L; 95% CI, -4.39-74.02 U/L) was observed between patients with severe MERS and non-severe MERS (Table 2). Limited studies reported the relationship between neurologic dysfunction or GI dysfunction and SARS or MERS severity. Unlike SARS (P<0.001); [123] and COVID-19, chronic cerebrovascular diseases was not a predictor for the severity of MERS (OR = 1.94; 95% CI, 0.69-5.43); (Supplementary Fig. 2-6).
Publications bias and Sensitivity analysis
Publication bias was noted in the following polled results: COPD (Begg=0.65, Egger=0.009), CKD (Begg=0.075, Egger=0.006), and headache (Begg=0.01, Egger=0.047) (Supplementary Table 2). The we performed trim-and-fill analysis. Although the direction of overall effects did not change, more articles should be included in future studies to reduce publication bias. Sensitivity analyses revealed no significant differences in the outcomes except for the pooled results of CLD, dizziness, nausea and/or vomiting and diarrhea (Supplementary Fig. 7).
DISCUSSION
In the present study, data from 73 studies were meta-analyzed and the following conclusions were drawn. Although COVID-19 spreads rapidly and has a high incidence rate, it has a relatively low CFR and CSR. The most common comorbidity was hypertension, followed by diabetes and CVD. The most common complication was ARDS, followed by ACI and shock. Elevated levels of LDH and myoglobin were observed in COVID-19 patients. The most common neurologic symptom was olfactory and/or taste disorders and the most dominant GI symptom was anorexia. A history of organ dysfunction and abnormal biomedical indicators of organ function are significant predictors of a poor prognosis for all of the three coronavirus infections. In addition, patients with severe COVID-19 infections are more likely to have some neurologic and GI symptoms. Finally, acute organ injury was more commonly observed in severe COVID-19 cases.
According to studies on COVID-19, the presence of comorbidities is a predictor of a poor outcome. It is important to evaluate the prevalence of comorbidities in COVID-19 patients. In the present meta-analysis, the overall proportion of patients with hypertension, diabetes, CVD, chronic GI diseases, chronic cerebrovascular diseases, COPD, CLD, and CKD was 19%, 10%, 8%, 7%, 3%, 2%, 3%, and 3%, respectively. However, the prevalence of these chronic diseases is considerably higher in the general population [139, 140]. Hence, we could not determine whether patients with comorbidities are more susceptible to COVID-19 infection.
However, we assuredly do know that patients with comorbidities such as hypertension, CVD, CKD and COPD, are vulnerable to developing severe disease, which is consistent with previous studies [7, 141]. It can be speculated that comorbidities influence COVID-19 through two mechanisms. First, comorbidities are more prevalent among individuals of advanced age. Innate immunity serves as the first line of defense against pathogen invasion, and successful mounting of type I interferon (IFN) response should be able to suppress viral replication at an early stage [142]. Aging has been reported to impair the capacity of plasmacytoid dendritic cells, which are the most important type of I IFN producing cells [143, 144]. When the innate immune response is not effective and a delayed-type I IFN response is mounted, the virus cannot be controlled in the early phase of infection and patients are more likely to develop a severe infection. Second, in SARS and MERS infection, the influx of hyperinflammatory cytokines and chemokines is the main cause of lethal outcomes [144, 145]. Huang et al. reported that in COVID-19, higher levels of inflammatory factors were more commonly seen in patients with severe COVID-19 than in those with non-severe COVID-19, suggesting that a cytokine storm was associated with disease severity [8]. Patients with various chronic diseases are already in a proinflammatory state with impaired immune function; hence, the infection can accelerate the inflammatory progress [146]. Therefore, patients with a history of organ dysfunction may have a greater risk of developing severe COVID-19.
Another key finding is that COVID-19 appears to target multiple organs and induces acute injury. Li et al. found that the condition of patients without AKI at admission could gradually worsen and AKI may be diagnosed during hospitalization [147]. Guo et al. reported that some patients without underlying CVD had elevated TnT levels [148]. In this study, further analysis indicated that the incidence of acute multiorgan injury was considerably higher in patients with severe COVID-19. Similar to SARS-CoV, SARS-CoV-2 uses angiotensin-converting enzyme 2 (ACE2) as the cell entry receptor [149]. Zhao et al. demonstrated that ACE2 was principally expressed in alveolar epithelial type II cells, suggesting that the lung could be the most vulnerable target organ. However, ACE2 is highly expressed in the heart, kidney, liver, brain, and digestive tract, which provides a means for the involvement of multiple organs in COVID-19 [150-152]. Immunostaining of lung tissues indicated that the Rp3 nucleocapsid protein (NP) of SARS-CoV-2 was prominently expressed on alveolar epithelial cells, and histopathological examination revealed all the features of diffuse alveolar damage [103, 153]. Diao et al. found that various degrees of acute tubular necrosis and viral infection-associated syncytia were observed in renal specimens of COVID-19 patients. Furthermore, the NP antigens of SARS-CoV-2 could be observed in kidney tissues [154]. Clusters of coronavirus particles with distinctive spikes were observed in the tubular epithelium and podocytes [155]. No substantial histological changes were identified in the heart [103, 156], however SARS-CoV-2 viral particles have been identified in cardiac tissue in some COVID-19 cases [157, 158]. Biopsy of liver tissues revealed moderate microvesicular steatosis and mild lobular and portal activity; however, the possibility of drug-induced acute liver injury cannot be ruled out [103]. It has been reported that liver injury observed in COVID-19 patients after admission may be caused by LPV/r treatment [104]. Notably, viral RNA was also detected in the liver tissues of COVID-19 patients [158]. Similar to SARS-CoV, SARS-CoV-2 might invade the central nervous system via the nose close to the olfactory epithelium [159]. This was supported by the presence of olfactory disorders in patients with COVID-19. Detectable viral RNA was identified in the brain tissues of some COVID-19 cases [158], and the presence of specific SARS-CoV-2 RNA in COVID-19 patients’ cerebrospinal fluid has also been confirmed [160]. The SARS-CoV-2 RNA and NP were detected in GI tissues from COVID-19 patients [161]. In addition, the successful isolation of SARS-CoV-2 from stool samples demonstrated the fact that there was GI infection [162]. These results suggested that regional viral replication could directly contribute to acute organ damage. Of note, inflammatory cellular infiltration is commonly observed in multiple organs, including the lung, heart, kidney, and liver. This suggests that viruses not only induce direct organ damage but also aggravate the injury through proinflammatory function or cytokine storms [103, 156, 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection.
In addition, clinicians should be equally alert to patients without organ dysfunction prior to admission. Guo et al. reported that patients with underlying CVD and normal TnT levels had a considerably more favorable outcome than in patients without CVD and with elevated TnT levels [148]. Therefore, it is reasonable to speculate that acute organ injury may play a greater role in the lethal outcome of COVID-19 than a history of organ dysfunction. These results indicate that clinicians should evaluate and prioritize COVID-19 patients according to the presence of organ dysfunction and the evidence of acute organ injury and initiate aggressive treatment. Multiorgan function biomarkers should be closely monitored for early warning and intervention.
SARS-CoV, MERS-CoV, and SARS-CoV-2 belong to the same genus and all are beta-CoVs. The comparison of genomic sequences revealed that the SARS-CoV-2 genome is 79% and 50% similar to SARS-CoV and MERS-CoV, respectively. SARS-CoV-2 contains additional gene regions, and the amino acid sequences of some SARS-CoV-2 proteins are only 68% similar to those of SARS-CoV [144, 163, 164]. It is reasonable to speculate that SARS-CoV-2 has similar clinical features and pathology as SARS-CoV and MERS-CoV; however, additional characteristics may yet be discovered. These findings reveal that all three coronaviruses might originate in bats prior to mutations. Subsequently they adapt to intermediate hosts and finally to humans [163, 165]. SARS-CoV and SARS-CoV-2 share the cell entry receptor of ACE2, while Dipeptidyl peptidase (DPP)-4 serves as the specific receptor for MERS-CoV [144, 166]. Similar to SARS and MERS, lower respiratory symptoms, including fever, cough, and fatigue, were commonly observed in patients with early-stage COVID-19, while the incidence of GI symptoms was relatively low [17, 141]. In the present study, a history of organ dysfunction was identified as the predictor of severe disease in all three coronaviruses. In addition, the pathological changes in the multiorgan tissues of COVID-19 patients significantly resemble those observed in SARS and MERS infection. This provides evidence for our work [167, 168]. Coronaviruses not only induce direct organ damage but also aggravate the injury through proinflammatory methods. On the basis of the information from previous studies, we found that SARS-CoV-2 shared similarities with SARS-CoV and/or MERS-CoV in various aspects, including genomic sequence, origin, entry receptor, clinical features, risk factors, and pathological processes. As no vaccine or specific treatment with confirmed results is available for treating COVID-19, and COVID-19 has a huge impact, clinical experience from SARS and MERS may provide some guidance regarding treatment strategies that may benefit COVID-19 patients.
Limitations
Our meta-analysis has several limitations. First, most of the included studies are retrospective studies with a low level of evidence. However, the quality of the majority of studies included in the meta-analysis was moderate or high. Second, most patients in our meta-analysis were Chinese, and hence, conclusions might not be applicable to patients in different countries. Finally, some patients in the included studies remain in the hospital, which results in missing data.
Conclusion
The present study successfully and systematically evaluated the relationship between multiorgan dysfunction and COVID-19 severity. Patients with a history of organ dysfunction have a greater risk of developing severe COVID-19 and in turn COVID-19 can promote acute multiorgan injury. Clinicians should increase their awareness regarding the monitoring of multiorgan function in hospitalized COVID-19 patients. Early detection and effective intervention to prevent multiorgan dysfunction may aid in reducing the number of deaths in these patients.
Supplementary Materials
The Supplemenantry data can be found online at: www.aginganddisease.org/EN/10.14336/AD.2020.0520.
Acknowledgements
This work was supported by the National Natural Science Foundation of China under contract (Nos. 31672290, 31100764, 30901874), the National Key Research and Development Program of China (2016YFD0500300), Zhejiang University Special Scientific Research Fund for COVID-19 Prevention and Control (2020XGZX033), Science and Technology Plan Project of Changsha (Nos. kq2001033, kq2001012), the Natural Science Foundation of Hunan Province, China (No. 2016JJ3180), Open-End Fund for the Valuable and Precision Instruments of Central South University (Nos. CSUZC2020043, CSUZC2019046).
Conflict of interest
The authors declare that they have no conflict of interest.
Potential Maternal and Infant Outcomes from (Wuhan) Coronavirus 2019-nCoV Infecting Pregnant Women: Lessons from SARS, MERS, and Other Human Coronavirus Infections
ZhengY, HuangZ, YingG, ZhangX, YeW, HuZ, et al. (2020).
Study of the lymphocyte change between COVID-19 and non-COVID-19 pneumonia cases suggesting other factors besides uncontrolled inflammation contributed to multi-organ injury
. medRxiv:2020.2002.2019.20024885.
[31]
LuH, AiJ, ShenY, LiY, LiT, ZhouX, et al. (2020).
A descriptive study of the impact of diseases control and prevention on the epidemics dynamics and clinical features of SARS-CoV-2 outbreak in Shanghai, lessons learned for metropolis epidemics prevention
. medRxiv:2020.2002.2019.20025031.
[32]
LeiL, Jian-yaG (2020).
Clinical characteristics of 51 patients discharged from hospital with COVID-19 in Chongqing,China
. medRxiv:2020.2002.2020.20025536.
[33]
ChenX, ZhengF, QingY, DingS, YangD, LeiC, et al. (2020).
Epidemiological and clinical features of 291 cases with coronavirus disease 2019 in areas adjacent to Hubei, China: a double-center observational study
. medRxiv:2020.2003.2003.20030353.
[34]
YangW, CaoQ, QinL, WangX, ChengZ, PanA, et al. (2020).
Clinical characteristics and imaging manifestations of the 2019 novel coronavirus disease (COVID-19):A multi-center study in Wenzhou city, Zhejiang, China
. J Infect, 80:388-393.
[35]
ChenN, ZhouM, DongX, QuJ, GongF, HanY, et al. (2020).
Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study
. Lancet, 395:507-513.
[36]
XuXW, WuXX, JiangXG, XuKJ, YingLJ, MaCL, et al. (2020).
Clinical findings in a group of patients infected with the 2019 novel coronavirus (SARS-Cov-2) outside of Wuhan, China: retrospective case series
. Bmj, 368:m606.
[37]
ShiH, HanX, JiangN, CaoY, AlwalidO, GuJ, et al. (2020).
Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: a descriptive study
. Lancet Infect Dis, 20:425-434.
[38]
ZhouF, YuT, DuR, FanG, LiuY, LiuZ, et al. (2020).
Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study
. Lancet, 395:1054-1062.
[39]
LiuK, FangYY, DengY, LiuW, WangMF, MaJP, et al. (2020).
Clinical characteristics of novel coronavirus cases in tertiary hospitals in Hubei Province
. Chin Med J (Engl), in press.
[40]
WuJ, LiuJ, ZhaoX, LiuC, WangW, WangD, et al. (2020).
Clinical Characteristics of Imported Cases of COVID-19 in Jiangsu Province: A Multicenter Descriptive Study
. Clin Infect Dis, in press.
[41]
LiuW, TaoZW, LeiW, Ming-LiY, KuiL, LingZ, et al. (2020).
Analysis of factors associated with disease outcomes in hospitalized patients with 2019 novel coronavirus disease
. Chin Med J (Engl), in press.
[42]
GuanW-j, LiangW-h, ZhaoY, LiangH-r, ChenZ-s, LiY-m, et al. (2020).
Comorbidity and its impact on 1,590 patients with COVID-19 in China: A Nationwide Analysis
. medRxiv:2020.2002.2025.20027664.
[43]
YangY, LuQ, LiuM, WangY, ZhangA, JalaliN, et al. (2020).
Epidemiological and clinical features of the 2019 novel coronavirus outbreak in China
. medRxiv:2020.2002.2010.20021675.
[44]
ZhangY and The Novel Coronavirus Pneumonia Emergency Response Epidemiology Team. (2020). [
The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China
]. Zhonghua Liu Xing Bing Xue Za Zhi, 41:145-151.
[45]
WanS, XiangY, FangW, ZhengY, LiB, HuY, et al. (2020).
Clinical features and treatment of COVID-19 patients in northeast Chongqing
. J Med Virol, in press.
[46]
XuX, YuC, QuJ, ZhangL, JiangS, HuangD, et al. (2020).
Imaging and clinical features of patients with 2019 novel coronavirus SARS-CoV-2
. Eur J Nucl Med Mol Imaging, 47:1275-1280.
[47]
QiD, YanX, TangX, PengJ, YuQ, FengL, et al. (2020).
Epidemiological and clinical features of 2019-nCoV acute respiratory disease cases in Chongqing municipality, China: a retrospective, descriptive, multiple-center study
. medRxiv:2020.2003.2001.20029397.
[48]
ZhaoW, YuS, ZhaX, WangN, PangQ, LiT, et al. (2020).
Clinical characteristics and durations of hospitalized patients with COVID-19 in Beijing: a retrospective cohort study
. medRxiv: 2020.2003.2013.20035436.
[49]
MaK-L, LiuZ-H, CaoC-f, LiuM-K, LiaoJ, ZouJ-B, et al. (2020).
COVID-19 Myocarditis and Severity Factors: An Adult Cohort Study
MahevasM, TranV-T, RoumierM, ChabrolA, PauleR, GuillaudC, et al. (2020).
No evidence of clinical efficacy of hydroxychloroquine in patients hospitalized for COVID-19 infection with oxygen requirement: results of a study using routinely collected data to emulate a target trial
de WildeAH, JochmansD, PosthumaCC, Zevenhoven-DobbeJC, van NieuwkoopS, BestebroerTM, et al. (2014).
Screening of an FDA-approved compound library identifies four small-molecule inhibitors of Middle East respiratory syndrome coronavirus replication in cell culture
WisniewskiA, KirchgesnerJ, SeksikP, LandmanC, BourrierA, Nion-LarmurierI, et al. (2020).
Increased incidence of systemic serious viral infections in patients with inflammatory bowel disease associates with active disease and use of thiopurines
. United European Gastroenterology Journal, 8:303-313.
NgDL, Al HosaniF, KeatingMK, GerberSI, JonesTL, MetcalfeMG, et al. (2016).
Clinicopathologic, Immunohistochemical, and Ultrastructural Findings of a Fatal Case of Middle East Respiratory Syndrome Coronavirus Infection in the United Arab Emirates, April 2014
... Coronaviruses are positive-stranded ribonucleic acid (+RNA) viruses belonging to the family Coronaviridae and order Nidovirales [1, 2]. Prior to December 2019, six coronavirus species had been identified and these primarily caused mild illness [2, 3]. However, in the past decades, two zoonotic coronaviruses, severe acute respiratory syndrome coronavirus (SARS-CoV) and Middle East respiratory syndrome coronavirus (MERS-CoV), resulted in severe and even fatal lower respiratory tract infections, with more than 8000 and 1500 confirmed cases and 10% and 37% case fatality rates (CFR), respectively [4, 5]. Although coronavirus infections have a huge effect, strategies to prevent and treat coronavirus infection are limited due to the lack of effective antiviral treatments [6]. ...
Epidemic and Emerging Coronaviruses (Severe Acute Respiratory Syndrome and Middle East Respiratory Syndrome)
2
2017
... Coronaviruses are positive-stranded ribonucleic acid (+RNA) viruses belonging to the family Coronaviridae and order Nidovirales [1, 2]. Prior to December 2019, six coronavirus species had been identified and these primarily caused mild illness [2, 3]. However, in the past decades, two zoonotic coronaviruses, severe acute respiratory syndrome coronavirus (SARS-CoV) and Middle East respiratory syndrome coronavirus (MERS-CoV), resulted in severe and even fatal lower respiratory tract infections, with more than 8000 and 1500 confirmed cases and 10% and 37% case fatality rates (CFR), respectively [4, 5]. Although coronavirus infections have a huge effect, strategies to prevent and treat coronavirus infection are limited due to the lack of effective antiviral treatments [6]. ...
... ]. Prior to December 2019, six coronavirus species had been identified and these primarily caused mild illness [2, 3]. However, in the past decades, two zoonotic coronaviruses, severe acute respiratory syndrome coronavirus (SARS-CoV) and Middle East respiratory syndrome coronavirus (MERS-CoV), resulted in severe and even fatal lower respiratory tract infections, with more than 8000 and 1500 confirmed cases and 10% and 37% case fatality rates (CFR), respectively [4, 5]. Although coronavirus infections have a huge effect, strategies to prevent and treat coronavirus infection are limited due to the lack of effective antiviral treatments [6]. ...
From SARS to MERS, Thrusting Coronaviruses into the Spotlight
1
2019
... Coronaviruses are positive-stranded ribonucleic acid (+RNA) viruses belonging to the family Coronaviridae and order Nidovirales [1, 2]. Prior to December 2019, six coronavirus species had been identified and these primarily caused mild illness [2, 3]. However, in the past decades, two zoonotic coronaviruses, severe acute respiratory syndrome coronavirus (SARS-CoV) and Middle East respiratory syndrome coronavirus (MERS-CoV), resulted in severe and even fatal lower respiratory tract infections, with more than 8000 and 1500 confirmed cases and 10% and 37% case fatality rates (CFR), respectively [4, 5]. Although coronavirus infections have a huge effect, strategies to prevent and treat coronavirus infection are limited due to the lack of effective antiviral treatments [6]. ...
SARS: prognosis, outcome and sequelae
1
2003
... Coronaviruses are positive-stranded ribonucleic acid (+RNA) viruses belonging to the family Coronaviridae and order Nidovirales [1, 2]. Prior to December 2019, six coronavirus species had been identified and these primarily caused mild illness [2, 3]. However, in the past decades, two zoonotic coronaviruses, severe acute respiratory syndrome coronavirus (SARS-CoV) and Middle East respiratory syndrome coronavirus (MERS-CoV), resulted in severe and even fatal lower respiratory tract infections, with more than 8000 and 1500 confirmed cases and 10% and 37% case fatality rates (CFR), respectively [4, 5]. Although coronavirus infections have a huge effect, strategies to prevent and treat coronavirus infection are limited due to the lack of effective antiviral treatments [6]. ...
Prevalence of Diabetes in the 2009 Influenza A (H1N1) and the Middle East Respiratory Syndrome Coronavirus: A Systematic Review and Meta-Analysis
1
2016
... Coronaviruses are positive-stranded ribonucleic acid (+RNA) viruses belonging to the family Coronaviridae and order Nidovirales [1, 2]. Prior to December 2019, six coronavirus species had been identified and these primarily caused mild illness [2, 3]. However, in the past decades, two zoonotic coronaviruses, severe acute respiratory syndrome coronavirus (SARS-CoV) and Middle East respiratory syndrome coronavirus (MERS-CoV), resulted in severe and even fatal lower respiratory tract infections, with more than 8000 and 1500 confirmed cases and 10% and 37% case fatality rates (CFR), respectively [4, 5]. Although coronavirus infections have a huge effect, strategies to prevent and treat coronavirus infection are limited due to the lack of effective antiviral treatments [6]. ...
Potential Maternal and Infant Outcomes from (Wuhan) Coronavirus 2019-nCoV Infecting Pregnant Women: Lessons from SARS, MERS, and Other Human Coronavirus Infections
1
2020
... Coronaviruses are positive-stranded ribonucleic acid (+RNA) viruses belonging to the family Coronaviridae and order Nidovirales [1, 2]. Prior to December 2019, six coronavirus species had been identified and these primarily caused mild illness [2, 3]. However, in the past decades, two zoonotic coronaviruses, severe acute respiratory syndrome coronavirus (SARS-CoV) and Middle East respiratory syndrome coronavirus (MERS-CoV), resulted in severe and even fatal lower respiratory tract infections, with more than 8000 and 1500 confirmed cases and 10% and 37% case fatality rates (CFR), respectively [4, 5]. Although coronavirus infections have a huge effect, strategies to prevent and treat coronavirus infection are limited due to the lack of effective antiviral treatments [6]. ...
Prevalence of comorbidities in the novel Wuhan coronavirus (COVID-19) infection: a systematic review and meta-analysis
2
2020
... At the beginning of December 2019, pneumonia due to an unknown cause was reported in a series of patients. On January 7, 2020, the cause was identified as a novel coronavirus infection. This virus was named SARS-CoV-2 by the World Health Organization (WHO). Similar to SARS-CoV and MERS-CoV, SARS-CoV-2 targets the respiratory tract and the dominant symptoms of COVID-19 at the beginning of the illness are fever, cough, fatigue, or myalgia [7, 8]. Although COVID-19 has a relatively low CFR, it is spreading rampantly, with more than four million confirmed cases, and it has affected the global economy and human health. ...
... However, we assuredly do know that patients with comorbidities such as hypertension, CVD, CKD and COPD, are vulnerable to developing severe disease, which is consistent with previous studies [7, 141]. It can be speculated that comorbidities influence COVID-19 through two mechanisms. First, comorbidities are more prevalent among individuals of advanced age. Innate immunity serves as the first line of defense against pathogen invasion, and successful mounting of type I interferon (IFN) response should be able to suppress viral replication at an early stage [142]. Aging has been reported to impair the capacity of plasmacytoid dendritic cells, which are the most important type of I IFN producing cells [143, 144]. When the innate immune response is not effective and a delayed-type I IFN response is mounted, the virus cannot be controlled in the early phase of infection and patients are more likely to develop a severe infection. Second, in SARS and MERS infection, the influx of hyperinflammatory cytokines and chemokines is the main cause of lethal outcomes [144, 145]. Huang et al. reported that in COVID-19, higher levels of inflammatory factors were more commonly seen in patients with severe COVID-19 than in those with non-severe COVID-19, suggesting that a cytokine storm was associated with disease severity [8]. Patients with various chronic diseases are already in a proinflammatory state with impaired immune function; hence, the infection can accelerate the inflammatory progress [146]. Therefore, patients with a history of organ dysfunction may have a greater risk of developing severe COVID-19. ...
Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China
4
2020
... At the beginning of December 2019, pneumonia due to an unknown cause was reported in a series of patients. On January 7, 2020, the cause was identified as a novel coronavirus infection. This virus was named SARS-CoV-2 by the World Health Organization (WHO). Similar to SARS-CoV and MERS-CoV, SARS-CoV-2 targets the respiratory tract and the dominant symptoms of COVID-19 at the beginning of the illness are fever, cough, fatigue, or myalgia [7, 8]. Although COVID-19 has a relatively low CFR, it is spreading rampantly, with more than four million confirmed cases, and it has affected the global economy and human health. ...
... Studies have suggested that COVID-19 leads to the development of severe pneumonia, other complications, and even death, especially in high-risk patients [9, 10]. To date, neither a vaccine nor a specific treatment with a confirmed result has been available to patients. Hence, effective methods to improve the outcomes in patients with severe COVID-19 may include the early prevention of SARS-CoV-2 infection in high-risk patients and the early monitoring and intervention regarding the parameters associated with disease severity. It has been reported that patients with diabetes, hypertension, and coronary heart diseases are 2.85, 3.05, and 21.40 times more likely to have a poor prognosis, respectively, than that in patients without these diseases [10]. In addition, elevated alanine aminotransferase (ALT), lactate dehydrogenase (LDH), high-sensitivity cardiac troponin I (hs-cTnI), and urea levels have been reported to be associated with disease severity [11, 12]. The incidence of complications, including acute respiratory distress syndrome (ARDS) and acute cardiac injury (ACI), is higher in patients with severe COVID-19 [8, 10]. These clinically relevant parameters are closely related to various organ functions in patients. Hence, we wanted to know whether patients with a history of organ dysfunction are more susceptible to COVID-19 infection and whether COVID-19 infection aggravates acute damage to various organs. Given the rapid spread of COVID-19 with no specific treatment available, it is urgent to analyze published and high-quality clinical studies to identify guidelines for the management of the patients. This study aimed to provide systematic evidence for the association between multiorgan dysfunction and COVID-19 severity and to compare differences in the indices of organ function among COVID-19, SARS, and MERS. In addition, based on the existing literature, we have provided certain treatment suggestions for patients with dysfunction of various organs. ...
... A total of 5037 relevant articles were identified by searching several online databases. Figure 1 presents the screening and selection process of the eligible trials. The characteristics of the included trials are listed in Supplementary Table 1. This meta-analysis included 73 studies [8, 11, 12, 14-83]. Among these studies, 54 were from China, 4 from Italy, 3 from The United States, 2 from The United Kingdom, 2 from France, 2 from Spain, and the remaining 6 from other countries. Clinical features of severe and non-severe COVID-19 cases were reported by 48 studies. The results of the quality assessments were presented in Supplementary Table 1. ...
... However, we assuredly do know that patients with comorbidities such as hypertension, CVD, CKD and COPD, are vulnerable to developing severe disease, which is consistent with previous studies [7, 141]. It can be speculated that comorbidities influence COVID-19 through two mechanisms. First, comorbidities are more prevalent among individuals of advanced age. Innate immunity serves as the first line of defense against pathogen invasion, and successful mounting of type I interferon (IFN) response should be able to suppress viral replication at an early stage [142]. Aging has been reported to impair the capacity of plasmacytoid dendritic cells, which are the most important type of I IFN producing cells [143, 144]. When the innate immune response is not effective and a delayed-type I IFN response is mounted, the virus cannot be controlled in the early phase of infection and patients are more likely to develop a severe infection. Second, in SARS and MERS infection, the influx of hyperinflammatory cytokines and chemokines is the main cause of lethal outcomes [144, 145]. Huang et al. reported that in COVID-19, higher levels of inflammatory factors were more commonly seen in patients with severe COVID-19 than in those with non-severe COVID-19, suggesting that a cytokine storm was associated with disease severity [8]. Patients with various chronic diseases are already in a proinflammatory state with impaired immune function; hence, the infection can accelerate the inflammatory progress [146]. Therefore, patients with a history of organ dysfunction may have a greater risk of developing severe COVID-19. ...
Platelet-to-lymphocyte ratio is associated with prognosis in patients with Corona Virus Disease-19
1
2020
... Studies have suggested that COVID-19 leads to the development of severe pneumonia, other complications, and even death, especially in high-risk patients [9, 10]. To date, neither a vaccine nor a specific treatment with a confirmed result has been available to patients. Hence, effective methods to improve the outcomes in patients with severe COVID-19 may include the early prevention of SARS-CoV-2 infection in high-risk patients and the early monitoring and intervention regarding the parameters associated with disease severity. It has been reported that patients with diabetes, hypertension, and coronary heart diseases are 2.85, 3.05, and 21.40 times more likely to have a poor prognosis, respectively, than that in patients without these diseases [10]. In addition, elevated alanine aminotransferase (ALT), lactate dehydrogenase (LDH), high-sensitivity cardiac troponin I (hs-cTnI), and urea levels have been reported to be associated with disease severity [11, 12]. The incidence of complications, including acute respiratory distress syndrome (ARDS) and acute cardiac injury (ACI), is higher in patients with severe COVID-19 [8, 10]. These clinically relevant parameters are closely related to various organ functions in patients. Hence, we wanted to know whether patients with a history of organ dysfunction are more susceptible to COVID-19 infection and whether COVID-19 infection aggravates acute damage to various organs. Given the rapid spread of COVID-19 with no specific treatment available, it is urgent to analyze published and high-quality clinical studies to identify guidelines for the management of the patients. This study aimed to provide systematic evidence for the association between multiorgan dysfunction and COVID-19 severity and to compare differences in the indices of organ function among COVID-19, SARS, and MERS. In addition, based on the existing literature, we have provided certain treatment suggestions for patients with dysfunction of various organs. ...
Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study
3
2020
... Studies have suggested that COVID-19 leads to the development of severe pneumonia, other complications, and even death, especially in high-risk patients [9, 10]. To date, neither a vaccine nor a specific treatment with a confirmed result has been available to patients. Hence, effective methods to improve the outcomes in patients with severe COVID-19 may include the early prevention of SARS-CoV-2 infection in high-risk patients and the early monitoring and intervention regarding the parameters associated with disease severity. It has been reported that patients with diabetes, hypertension, and coronary heart diseases are 2.85, 3.05, and 21.40 times more likely to have a poor prognosis, respectively, than that in patients without these diseases [10]. In addition, elevated alanine aminotransferase (ALT), lactate dehydrogenase (LDH), high-sensitivity cardiac troponin I (hs-cTnI), and urea levels have been reported to be associated with disease severity [11, 12]. The incidence of complications, including acute respiratory distress syndrome (ARDS) and acute cardiac injury (ACI), is higher in patients with severe COVID-19 [8, 10]. These clinically relevant parameters are closely related to various organ functions in patients. Hence, we wanted to know whether patients with a history of organ dysfunction are more susceptible to COVID-19 infection and whether COVID-19 infection aggravates acute damage to various organs. Given the rapid spread of COVID-19 with no specific treatment available, it is urgent to analyze published and high-quality clinical studies to identify guidelines for the management of the patients. This study aimed to provide systematic evidence for the association between multiorgan dysfunction and COVID-19 severity and to compare differences in the indices of organ function among COVID-19, SARS, and MERS. In addition, based on the existing literature, we have provided certain treatment suggestions for patients with dysfunction of various organs. ...
... ]. To date, neither a vaccine nor a specific treatment with a confirmed result has been available to patients. Hence, effective methods to improve the outcomes in patients with severe COVID-19 may include the early prevention of SARS-CoV-2 infection in high-risk patients and the early monitoring and intervention regarding the parameters associated with disease severity. It has been reported that patients with diabetes, hypertension, and coronary heart diseases are 2.85, 3.05, and 21.40 times more likely to have a poor prognosis, respectively, than that in patients without these diseases [10]. In addition, elevated alanine aminotransferase (ALT), lactate dehydrogenase (LDH), high-sensitivity cardiac troponin I (hs-cTnI), and urea levels have been reported to be associated with disease severity [11, 12]. The incidence of complications, including acute respiratory distress syndrome (ARDS) and acute cardiac injury (ACI), is higher in patients with severe COVID-19 [8, 10]. These clinically relevant parameters are closely related to various organ functions in patients. Hence, we wanted to know whether patients with a history of organ dysfunction are more susceptible to COVID-19 infection and whether COVID-19 infection aggravates acute damage to various organs. Given the rapid spread of COVID-19 with no specific treatment available, it is urgent to analyze published and high-quality clinical studies to identify guidelines for the management of the patients. This study aimed to provide systematic evidence for the association between multiorgan dysfunction and COVID-19 severity and to compare differences in the indices of organ function among COVID-19, SARS, and MERS. In addition, based on the existing literature, we have provided certain treatment suggestions for patients with dysfunction of various organs. ...
... , 10]. These clinically relevant parameters are closely related to various organ functions in patients. Hence, we wanted to know whether patients with a history of organ dysfunction are more susceptible to COVID-19 infection and whether COVID-19 infection aggravates acute damage to various organs. Given the rapid spread of COVID-19 with no specific treatment available, it is urgent to analyze published and high-quality clinical studies to identify guidelines for the management of the patients. This study aimed to provide systematic evidence for the association between multiorgan dysfunction and COVID-19 severity and to compare differences in the indices of organ function among COVID-19, SARS, and MERS. In addition, based on the existing literature, we have provided certain treatment suggestions for patients with dysfunction of various organs. ...
CT manifestations of coronavirus disease-2019: A retrospective analysis of 73 cases by disease severity
2
2020
... Studies have suggested that COVID-19 leads to the development of severe pneumonia, other complications, and even death, especially in high-risk patients [9, 10]. To date, neither a vaccine nor a specific treatment with a confirmed result has been available to patients. Hence, effective methods to improve the outcomes in patients with severe COVID-19 may include the early prevention of SARS-CoV-2 infection in high-risk patients and the early monitoring and intervention regarding the parameters associated with disease severity. It has been reported that patients with diabetes, hypertension, and coronary heart diseases are 2.85, 3.05, and 21.40 times more likely to have a poor prognosis, respectively, than that in patients without these diseases [10]. In addition, elevated alanine aminotransferase (ALT), lactate dehydrogenase (LDH), high-sensitivity cardiac troponin I (hs-cTnI), and urea levels have been reported to be associated with disease severity [11, 12]. The incidence of complications, including acute respiratory distress syndrome (ARDS) and acute cardiac injury (ACI), is higher in patients with severe COVID-19 [8, 10]. These clinically relevant parameters are closely related to various organ functions in patients. Hence, we wanted to know whether patients with a history of organ dysfunction are more susceptible to COVID-19 infection and whether COVID-19 infection aggravates acute damage to various organs. Given the rapid spread of COVID-19 with no specific treatment available, it is urgent to analyze published and high-quality clinical studies to identify guidelines for the management of the patients. This study aimed to provide systematic evidence for the association between multiorgan dysfunction and COVID-19 severity and to compare differences in the indices of organ function among COVID-19, SARS, and MERS. In addition, based on the existing literature, we have provided certain treatment suggestions for patients with dysfunction of various organs. ...
... A total of 5037 relevant articles were identified by searching several online databases. Figure 1 presents the screening and selection process of the eligible trials. The characteristics of the included trials are listed in Supplementary Table 1. This meta-analysis included 73 studies [8, 11, 12, 14-83]. Among these studies, 54 were from China, 4 from Italy, 3 from The United States, 2 from The United Kingdom, 2 from France, 2 from Spain, and the remaining 6 from other countries. Clinical features of severe and non-severe COVID-19 cases were reported by 48 studies. The results of the quality assessments were presented in Supplementary Table 1. ...
Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China
2
2020
... Studies have suggested that COVID-19 leads to the development of severe pneumonia, other complications, and even death, especially in high-risk patients [9, 10]. To date, neither a vaccine nor a specific treatment with a confirmed result has been available to patients. Hence, effective methods to improve the outcomes in patients with severe COVID-19 may include the early prevention of SARS-CoV-2 infection in high-risk patients and the early monitoring and intervention regarding the parameters associated with disease severity. It has been reported that patients with diabetes, hypertension, and coronary heart diseases are 2.85, 3.05, and 21.40 times more likely to have a poor prognosis, respectively, than that in patients without these diseases [10]. In addition, elevated alanine aminotransferase (ALT), lactate dehydrogenase (LDH), high-sensitivity cardiac troponin I (hs-cTnI), and urea levels have been reported to be associated with disease severity [11, 12]. The incidence of complications, including acute respiratory distress syndrome (ARDS) and acute cardiac injury (ACI), is higher in patients with severe COVID-19 [8, 10]. These clinically relevant parameters are closely related to various organ functions in patients. Hence, we wanted to know whether patients with a history of organ dysfunction are more susceptible to COVID-19 infection and whether COVID-19 infection aggravates acute damage to various organs. Given the rapid spread of COVID-19 with no specific treatment available, it is urgent to analyze published and high-quality clinical studies to identify guidelines for the management of the patients. This study aimed to provide systematic evidence for the association between multiorgan dysfunction and COVID-19 severity and to compare differences in the indices of organ function among COVID-19, SARS, and MERS. In addition, based on the existing literature, we have provided certain treatment suggestions for patients with dysfunction of various organs. ...
... A total of 5037 relevant articles were identified by searching several online databases. Figure 1 presents the screening and selection process of the eligible trials. The characteristics of the included trials are listed in Supplementary Table 1. This meta-analysis included 73 studies [8, 11, 12, 14-83]. Among these studies, 54 were from China, 4 from Italy, 3 from The United States, 2 from The United Kingdom, 2 from France, 2 from Spain, and the remaining 6 from other countries. Clinical features of severe and non-severe COVID-19 cases were reported by 48 studies. The results of the quality assessments were presented in Supplementary Table 1. ...
Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range
1
2014
... The weighted mean difference (WMD) and odds ratio (OR) were used to compare continuous and dichotomous variables, respectively. All the results were reported with 95% confidence intervals (CIs). Median (range) or median (interquartile range [IQR]) will be converted to the form of mean (standard deviation [SD]) [13]. We pooled the effect estimates of the outcomes by using fixed-effect models. A random effect model was used when significant heterogeneity was detected. Heterogeneity was assessed by using the I2 value, and an I2 of >50% was considered significant. The sensitivity analyses were made by excluding one study at a time to observe the change of the effects on the outcomes. Egger’s test, and Begg’s test (P < 0.10) were used to suggest the possible publication bias of outcomes. We performed all statistical analyses with the STATA 12.0 statistical software package (StataCoporation, College Station, Texas, USA). ...
Platelet-to-lymphocyte ratio is associated with prognosis in patients with coronavirus disease-19
1
2020
... A total of 5037 relevant articles were identified by searching several online databases. Figure 1 presents the screening and selection process of the eligible trials. The characteristics of the included trials are listed in Supplementary Table 1. This meta-analysis included 73 studies [8, 11, 12, 14-83]. Among these studies, 54 were from China, 4 from Italy, 3 from The United States, 2 from The United Kingdom, 2 from France, 2 from Spain, and the remaining 6 from other countries. Clinical features of severe and non-severe COVID-19 cases were reported by 48 studies. The results of the quality assessments were presented in Supplementary Table 1. ...
Relation Between Chest CT Findings and Clinical Conditions of Coronavirus Disease (COVID-19) Pneumonia: A Multicenter Study
0
2020
Clinical and computed tomographic imaging features of novel coronavirus pneumonia caused by SARS-CoV-2
0
2020
Clinical Characteristics of Coronavirus Disease 2019 in China
1
2020
... SARS-CoV, MERS-CoV, and SARS-CoV-2 belong to the same genus and all are beta-CoVs. The comparison of genomic sequences revealed that the SARS-CoV-2 genome is 79% and 50% similar to SARS-CoV and MERS-CoV, respectively. SARS-CoV-2 contains additional gene regions, and the amino acid sequences of some SARS-CoV-2 proteins are only 68% similar to those of SARS-CoV [144, 163, 164]. It is reasonable to speculate that SARS-CoV-2 has similar clinical features and pathology as SARS-CoV and MERS-CoV; however, additional characteristics may yet be discovered. These findings reveal that all three coronaviruses might originate in bats prior to mutations. Subsequently they adapt to intermediate hosts and finally to humans [163, 165]. SARS-CoV and SARS-CoV-2 share the cell entry receptor of ACE2, while Dipeptidyl peptidase (DPP)-4 serves as the specific receptor for MERS-CoV [144, 166]. Similar to SARS and MERS, lower respiratory symptoms, including fever, cough, and fatigue, were commonly observed in patients with early-stage COVID-19, while the incidence of GI symptoms was relatively low [17, 141]. In the present study, a history of organ dysfunction was identified as the predictor of severe disease in all three coronaviruses. In addition, the pathological changes in the multiorgan tissues of COVID-19 patients significantly resemble those observed in SARS and MERS infection. This provides evidence for our work [167, 168]. Coronaviruses not only induce direct organ damage but also aggravate the injury through proinflammatory methods. On the basis of the information from previous studies, we found that SARS-CoV-2 shared similarities with SARS-CoV and/or MERS-CoV in various aspects, including genomic sequence, origin, entry receptor, clinical features, risk factors, and pathological processes. As no vaccine or specific treatment with confirmed results is available for treating COVID-19, and COVID-19 has a huge impact, clinical experience from SARS and MERS may provide some guidance regarding treatment strategies that may benefit COVID-19 patients. ...
The Clinical and Chest CT Features Associated with Severe and Critical COVID-19 Pneumonia
0
2020
Epidemiologic and Clinical Characteristics of 91 Hospitalized Patients with COVID-19 in Zhejiang, China: A retrospective, multi-centre case series
0
2020
Clinical features and outcomes of 221 patients with COVID-19 in Wuhan, China
0
2020
Diagnostic Utility of Clinical Laboratory Data Determinations for Patients with the Severe COVID-19
0
2020
Non-severe vs severe symptomatic COVID-19: 104 cases from the outbreak on the cruise ship “Diamond Princess” in Japan
0
2020
Clinical Features of Patients Infected with the 2019 Novel Coronavirus (COVID-19) in Shanghai, China
0
2020
Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China
0
2020
Dysregulation of immune response in patients with COVID-19 in Wuhan, China
0
2020
Clinical characteristics of refractory COVID-19 pneumonia in Wuhan, China
0
2020
Longitudinal characteristics of lymphocyte responses and cytokine profiles in the peripheral blood of SARS-CoV-2 infected patients
0
2020
Clinical and immunologic features in severe and moderate forms of Coronavirus Disease 2019
0
2020
COVID-19 in a Designated Infectious Diseases HospitalOutside Hubei Province, China
1
2020
... We analyzed the relationship between liver dysfunction and COVID-19 severity. CLD was a significant predictor of COVID-19 severity (OR = 1.48; 95% CI, 1.09-2.01). Significant differences in ALT (WMD = 7.11 U/L; 95% CI, 5.47-8.75 U/L), aspartate aminotransferase (AST; WMD = 16.10 U/L; 95% CI, 14.00-18.20 U/L), and total bilirubin (WMD = 2.75 mmol/L; 95% CI, 2.11-3.40 mmol/L) were observed in patients with severe and non-severe COVID-19. One study specifically presented a higher incidence of acute liver injury in patients with severe COVID-19 as compared with that in patients with non-severe COVID-19. This is consistent with laboratory indicators [29] (Fig. 6). ...
Study of the lymphocyte change between COVID-19 and non-COVID-19 pneumonia cases suggesting other factors besides uncontrolled inflammation contributed to multi-organ injury
0
2020
A descriptive study of the impact of diseases control and prevention on the epidemics dynamics and clinical features of SARS-CoV-2 outbreak in Shanghai, lessons learned for metropolis epidemics prevention
0
2020
Clinical characteristics of 51 patients discharged from hospital with COVID-19 in Chongqing,China
0
2020
Epidemiological and clinical features of 291 cases with coronavirus disease 2019 in areas adjacent to Hubei, China: a double-center observational study
0
2020
Clinical characteristics and imaging manifestations of the 2019 novel coronavirus disease (COVID-19):A multi-center study in Wenzhou city, Zhejiang, China
0
2020
Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study
0
2020
Clinical findings in a group of patients infected with the 2019 novel coronavirus (SARS-Cov-2) outside of Wuhan, China: retrospective case series
0
2020
Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: a descriptive study
0
2020
Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study
0
2020
Clinical characteristics of novel coronavirus cases in tertiary hospitals in Hubei Province
0
2020
Clinical Characteristics of Imported Cases of COVID-19 in Jiangsu Province: A Multicenter Descriptive Study
0
2020
Analysis of factors associated with disease outcomes in hospitalized patients with 2019 novel coronavirus disease
0
2020
Comorbidity and its impact on 1,590 patients with COVID-19 in China: A Nationwide Analysis
0
2020
Epidemiological and clinical features of the 2019 novel coronavirus outbreak in China
0
2020
The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China
0
2020
Clinical features and treatment of COVID-19 patients in northeast Chongqing
0
2020
Imaging and clinical features of patients with 2019 novel coronavirus SARS-CoV-2
0
2020
Epidemiological and clinical features of 2019-nCoV acute respiratory disease cases in Chongqing municipality, China: a retrospective, descriptive, multiple-center study
0
2020
Clinical characteristics and durations of hospitalized patients with COVID-19 in Beijing: a retrospective cohort study
0
2020
COVID-19 Myocarditis and Severity Factors: An Adult Cohort Study
0
2020
Metabolic disturbances and inflammatory dysfunction predict severity of coronavirus disease 2019 (COVID-19): a retrospective study
0
2020
Risk Factors Associated with Clinical Outcomes in 323 COVID-19 Hospitalized Patients in Wuhan, China
0
2020
Factors associated with hospitalization and critical illness among 4,103 patients with COVID-19 disease in New York City
0
2020
Anosmia and dysgeusia in patients with mild SARS-CoV-2 infection
0
2020
A cohort study of 223 patients explores the clinical risk factors for the severity diagnosis of COVID-19
0
2020
Cluster of COVID-19 in northern France: A retrospective closed cohort study
0
2020
Clinical Characteristics of Hospitalized Covid-19 Patients in New York City
0
2020
Gastrointestinal symptoms as Covid-19 onset in hospitalized Italian patients
0
2020
Features of 16,749 hospitalised UK patients with COVID-19 using the ISARIC WHO Clinical Characterisation Protocol
0
2020
A cohort of patients with COVID-19 in a major teaching hospital in Europe
0
2020
Objective Olfactory Evaluation of Self-reported Olfactory Dysfunction in a Case Series of 86 COVID-19 Patients
0
2020
Myocardial characteristics as the prognosis for COVID-19 patients
0
2020
Effect of underlying comorbidities on the infection and severity of COVID-19 in South Korea
0
2020
Clinical characteristics of 161 cases of corona virus disease 2019 (COVID-19) in Changsha
0
2020
Clinical Features of 69 Cases with Coronavirus Disease 2019 in Wuhan, China
0
2020
Self-reported olfactory and taste disorders in SARS-CoV-2 patients: a cross-sectional study
0
2020
Olfactory and Gustatory Dysfunction in Coronavirus Disease 19 (COVID-19)
0
2020
Acute-onset smell and taste disorders in the context of COVID-19: a pilot multicentre polymerase chain reaction based case-control study
0
2020
New onset acute symptomatic seizure and risk factors in coronavirus disease 2019: A retrospective multicenter study
0
2020
Clinical characteristics of coronavirus disease (COVID-19) early findings from a teaching hospital in Pavia, North Italy, 21 to 28 February 2020
0
2020
Objective evaluation of anosmia and ageusia in COVID-19 patients: Single-center experience on 72 cases
0
2020
Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China
0
2020
Clinical Features of Patients with Coronavirus Disease 2019 (COVID-19) from a Designated Hospital in Beijing, China
0
2020
Clinical and Epidemiological Characteristics of 1,420 European Patients with mild-to-moderate Coronavirus Disease 2019
0
2020
Liver impairment in COVID-19 patients: A retrospective analysis of 115 cases from a single centre in Wuhan city, China
0
2020
Epidemiological characteristics and clinical features of 32 critical and 67 noncritical cases of COVID-19 in Chengdu
0
2020
Epidemiological and clinical features of 125 Hospitalized Patients with COVID-19 in Fuyang, Anhui, China
0
2020
Predictive factors for disease progression in hospitalized patients with coronavirus disease 2019 in Wuhan, China
0
2020
Prevalence and Characteristics of Gastrointestinal Symptoms in Patients with SARS-CoV-2 Infection in the United States: A Multicenter Cohort Study
0
2020
Clinical features of 95 sequential hospitalised patients with novel coronavirus 2019 disease (COVID-19), the first UK cohort
0
2020
Clinical findings of patients with coronavirus disease 2019 in Jiangsu province, China: A retrospective, multi-center study
0
2020
COVID-19 with Different Severity: A Multi-center Study of Clinical Features
0
2020
Real-time tracking of self-reported symptoms to predict potential COVID-19
0
2020
CT quantification of pneumonia lesions in early days predicts progression to severe illness in a cohort of COVID-19 patients
1
2020
... A total of 5037 relevant articles were identified by searching several online databases. Figure 1 presents the screening and selection process of the eligible trials. The characteristics of the included trials are listed in Supplementary Table 1. This meta-analysis included 73 studies [8, 11, 12, 14-83]. Among these studies, 54 were from China, 4 from Italy, 3 from The United States, 2 from The United Kingdom, 2 from France, 2 from Spain, and the remaining 6 from other countries. Clinical features of severe and non-severe COVID-19 cases were reported by 48 studies. The results of the quality assessments were presented in Supplementary Table 1. ...
Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro
1
2020
... In the preclinical in vitro studies, chloroquine (CQ) was found to inhibit SARS-CoV-2 activity [84]. Hydroxychloroquine (HCQ), a derivative of CQ, was found to be more potent than CQ in vitro. In addition, researchers have confirmed the clinical benefits of CQ for SARS [85]. A randomized clinical trial found that HCQ significantly shortened the time to clinical recovery and promoted pneumonia absorption among COVID-19 patients [86]. Therefore, the guidelines recommend that the administration of CQ/HCQ may help to improve the clinical outcomes of COVID-19 patients. However, the efficiency and safety of CQ and HCQ for treating COVID-19 remain uncertain due to recent controversial results [87], especially its’ potential cardiac toxicity. CQ/HCQ alone can cause QT prolongation and is known to cause torsades de pointes, especially among patients with a history of cardiac dysfunction and when administered in combination with other drugs such as lopinavir/ritonavir (LPV/r); [88]. It was reported that 30% of patients treated with HCQ + azithromycin developed new QT prolongation of > 40 ms [89]. Therefore, we strongly recommend close monitoring of electrocardiograms with QTc evaluation and correction of any electrolyte imbalance prior to administering CQ/HCQ [90]. Non-essential QT-prolonging drugs, including LPV/r, should be avoided in patients with a history of cardiac dysfunction. ...
Chloroquine analogues in drug discovery: new directions of uses, mechanisms of actions and toxic manifestations from malaria to multifarious diseases
1
2015
... In the preclinical in vitro studies, chloroquine (CQ) was found to inhibit SARS-CoV-2 activity [84]. Hydroxychloroquine (HCQ), a derivative of CQ, was found to be more potent than CQ in vitro. In addition, researchers have confirmed the clinical benefits of CQ for SARS [85]. A randomized clinical trial found that HCQ significantly shortened the time to clinical recovery and promoted pneumonia absorption among COVID-19 patients [86]. Therefore, the guidelines recommend that the administration of CQ/HCQ may help to improve the clinical outcomes of COVID-19 patients. However, the efficiency and safety of CQ and HCQ for treating COVID-19 remain uncertain due to recent controversial results [87], especially its’ potential cardiac toxicity. CQ/HCQ alone can cause QT prolongation and is known to cause torsades de pointes, especially among patients with a history of cardiac dysfunction and when administered in combination with other drugs such as lopinavir/ritonavir (LPV/r); [88]. It was reported that 30% of patients treated with HCQ + azithromycin developed new QT prolongation of > 40 ms [89]. Therefore, we strongly recommend close monitoring of electrocardiograms with QTc evaluation and correction of any electrolyte imbalance prior to administering CQ/HCQ [90]. Non-essential QT-prolonging drugs, including LPV/r, should be avoided in patients with a history of cardiac dysfunction. ...
Efficacy of hydroxychloroquine in patients with COVID-19: results of a randomized clinical trial
1
2020
... In the preclinical in vitro studies, chloroquine (CQ) was found to inhibit SARS-CoV-2 activity [84]. Hydroxychloroquine (HCQ), a derivative of CQ, was found to be more potent than CQ in vitro. In addition, researchers have confirmed the clinical benefits of CQ for SARS [85]. A randomized clinical trial found that HCQ significantly shortened the time to clinical recovery and promoted pneumonia absorption among COVID-19 patients [86]. Therefore, the guidelines recommend that the administration of CQ/HCQ may help to improve the clinical outcomes of COVID-19 patients. However, the efficiency and safety of CQ and HCQ for treating COVID-19 remain uncertain due to recent controversial results [87], especially its’ potential cardiac toxicity. CQ/HCQ alone can cause QT prolongation and is known to cause torsades de pointes, especially among patients with a history of cardiac dysfunction and when administered in combination with other drugs such as lopinavir/ritonavir (LPV/r); [88]. It was reported that 30% of patients treated with HCQ + azithromycin developed new QT prolongation of > 40 ms [89]. Therefore, we strongly recommend close monitoring of electrocardiograms with QTc evaluation and correction of any electrolyte imbalance prior to administering CQ/HCQ [90]. Non-essential QT-prolonging drugs, including LPV/r, should be avoided in patients with a history of cardiac dysfunction. ...
No evidence of clinical efficacy of hydroxychloroquine in patients hospitalized for COVID-19 infection with oxygen requirement: results of a study using routinely collected data to emulate a target trial
1
2020
... In the preclinical in vitro studies, chloroquine (CQ) was found to inhibit SARS-CoV-2 activity [84]. Hydroxychloroquine (HCQ), a derivative of CQ, was found to be more potent than CQ in vitro. In addition, researchers have confirmed the clinical benefits of CQ for SARS [85]. A randomized clinical trial found that HCQ significantly shortened the time to clinical recovery and promoted pneumonia absorption among COVID-19 patients [86]. Therefore, the guidelines recommend that the administration of CQ/HCQ may help to improve the clinical outcomes of COVID-19 patients. However, the efficiency and safety of CQ and HCQ for treating COVID-19 remain uncertain due to recent controversial results [87], especially its’ potential cardiac toxicity. CQ/HCQ alone can cause QT prolongation and is known to cause torsades de pointes, especially among patients with a history of cardiac dysfunction and when administered in combination with other drugs such as lopinavir/ritonavir (LPV/r); [88]. It was reported that 30% of patients treated with HCQ + azithromycin developed new QT prolongation of > 40 ms [89]. Therefore, we strongly recommend close monitoring of electrocardiograms with QTc evaluation and correction of any electrolyte imbalance prior to administering CQ/HCQ [90]. Non-essential QT-prolonging drugs, including LPV/r, should be avoided in patients with a history of cardiac dysfunction. ...
Diagnostic pitfalls and laboratory test interference after hydroxychloroquine intoxication: A case report
1
2019
... In the preclinical in vitro studies, chloroquine (CQ) was found to inhibit SARS-CoV-2 activity [84]. Hydroxychloroquine (HCQ), a derivative of CQ, was found to be more potent than CQ in vitro. In addition, researchers have confirmed the clinical benefits of CQ for SARS [85]. A randomized clinical trial found that HCQ significantly shortened the time to clinical recovery and promoted pneumonia absorption among COVID-19 patients [86]. Therefore, the guidelines recommend that the administration of CQ/HCQ may help to improve the clinical outcomes of COVID-19 patients. However, the efficiency and safety of CQ and HCQ for treating COVID-19 remain uncertain due to recent controversial results [87], especially its’ potential cardiac toxicity. CQ/HCQ alone can cause QT prolongation and is known to cause torsades de pointes, especially among patients with a history of cardiac dysfunction and when administered in combination with other drugs such as lopinavir/ritonavir (LPV/r); [88]. It was reported that 30% of patients treated with HCQ + azithromycin developed new QT prolongation of > 40 ms [89]. Therefore, we strongly recommend close monitoring of electrocardiograms with QTc evaluation and correction of any electrolyte imbalance prior to administering CQ/HCQ [90]. Non-essential QT-prolonging drugs, including LPV/r, should be avoided in patients with a history of cardiac dysfunction. ...
QT Interval Prolongation and Torsade De Pointes in Patients with COVID-19 treated with Hydroxychloroquine/Azithromycin
1
2020
... In the preclinical in vitro studies, chloroquine (CQ) was found to inhibit SARS-CoV-2 activity [84]. Hydroxychloroquine (HCQ), a derivative of CQ, was found to be more potent than CQ in vitro. In addition, researchers have confirmed the clinical benefits of CQ for SARS [85]. A randomized clinical trial found that HCQ significantly shortened the time to clinical recovery and promoted pneumonia absorption among COVID-19 patients [86]. Therefore, the guidelines recommend that the administration of CQ/HCQ may help to improve the clinical outcomes of COVID-19 patients. However, the efficiency and safety of CQ and HCQ for treating COVID-19 remain uncertain due to recent controversial results [87], especially its’ potential cardiac toxicity. CQ/HCQ alone can cause QT prolongation and is known to cause torsades de pointes, especially among patients with a history of cardiac dysfunction and when administered in combination with other drugs such as lopinavir/ritonavir (LPV/r); [88]. It was reported that 30% of patients treated with HCQ + azithromycin developed new QT prolongation of > 40 ms [89]. Therefore, we strongly recommend close monitoring of electrocardiograms with QTc evaluation and correction of any electrolyte imbalance prior to administering CQ/HCQ [90]. Non-essential QT-prolonging drugs, including LPV/r, should be avoided in patients with a history of cardiac dysfunction. ...
Of chloroquine and COVID-19
1
2020
... In the preclinical in vitro studies, chloroquine (CQ) was found to inhibit SARS-CoV-2 activity [84]. Hydroxychloroquine (HCQ), a derivative of CQ, was found to be more potent than CQ in vitro. In addition, researchers have confirmed the clinical benefits of CQ for SARS [85]. A randomized clinical trial found that HCQ significantly shortened the time to clinical recovery and promoted pneumonia absorption among COVID-19 patients [86]. Therefore, the guidelines recommend that the administration of CQ/HCQ may help to improve the clinical outcomes of COVID-19 patients. However, the efficiency and safety of CQ and HCQ for treating COVID-19 remain uncertain due to recent controversial results [87], especially its’ potential cardiac toxicity. CQ/HCQ alone can cause QT prolongation and is known to cause torsades de pointes, especially among patients with a history of cardiac dysfunction and when administered in combination with other drugs such as lopinavir/ritonavir (LPV/r); [88]. It was reported that 30% of patients treated with HCQ + azithromycin developed new QT prolongation of > 40 ms [89]. Therefore, we strongly recommend close monitoring of electrocardiograms with QTc evaluation and correction of any electrolyte imbalance prior to administering CQ/HCQ [90]. Non-essential QT-prolonging drugs, including LPV/r, should be avoided in patients with a history of cardiac dysfunction. ...
Kidney disease is associated with in-hospital death of patients with COVID-19
1
2020
... The present study revealed that the overall proportion of AKI was 4% (95% CI, 1%-7%) and AKI was associated with in-hospital mortality of COVID-19 patients [91]. According to the latest treatment protocol (Pilot Version 7) issued by the Chinese Health Commission, continuous renal replacement therapy (CRRT) is recommended for patients with severe COVID-19 and renal damage, especially for those with stage 3 AKI. CRRT removes inflammatory cytokines to regulate renal metabolic adaptation and improves kidney energy balance to protect the kidneys in patients with AKI [92]. Wang et al. suggested that COVID-19 patients with renal dysfunction should be monitored regularly. Once acute kidney failure develops, potential interventions, including CRRT, should be immediately initiated to protect renal function [93]. However, CRRT intensity should be carefully determined. A study indicated that higher-intensity CRRT treatment did not reduce mortality in patients with severe COVID-19 and AKI as compared with that in the control group [94]. ...
How Does Continuous Renal Replacement Therapy Affect Septic Acute Kidney Injury?
1
2018
... The present study revealed that the overall proportion of AKI was 4% (95% CI, 1%-7%) and AKI was associated with in-hospital mortality of COVID-19 patients [91]. According to the latest treatment protocol (Pilot Version 7) issued by the Chinese Health Commission, continuous renal replacement therapy (CRRT) is recommended for patients with severe COVID-19 and renal damage, especially for those with stage 3 AKI. CRRT removes inflammatory cytokines to regulate renal metabolic adaptation and improves kidney energy balance to protect the kidneys in patients with AKI [92]. Wang et al. suggested that COVID-19 patients with renal dysfunction should be monitored regularly. Once acute kidney failure develops, potential interventions, including CRRT, should be immediately initiated to protect renal function [93]. However, CRRT intensity should be carefully determined. A study indicated that higher-intensity CRRT treatment did not reduce mortality in patients with severe COVID-19 and AKI as compared with that in the control group [94]. ...
Coronavirus Disease 19 Infection Does Not Result in Acute Kidney Injury: An Analysis of 116 Hospitalized Patients from Wuhan, China
1
2020
... The present study revealed that the overall proportion of AKI was 4% (95% CI, 1%-7%) and AKI was associated with in-hospital mortality of COVID-19 patients [91]. According to the latest treatment protocol (Pilot Version 7) issued by the Chinese Health Commission, continuous renal replacement therapy (CRRT) is recommended for patients with severe COVID-19 and renal damage, especially for those with stage 3 AKI. CRRT removes inflammatory cytokines to regulate renal metabolic adaptation and improves kidney energy balance to protect the kidneys in patients with AKI [92]. Wang et al. suggested that COVID-19 patients with renal dysfunction should be monitored regularly. Once acute kidney failure develops, potential interventions, including CRRT, should be immediately initiated to protect renal function [93]. However, CRRT intensity should be carefully determined. A study indicated that higher-intensity CRRT treatment did not reduce mortality in patients with severe COVID-19 and AKI as compared with that in the control group [94]. ...
Intensity of continuous renal-replacement therapy in critically ill patients
1
2009
... The present study revealed that the overall proportion of AKI was 4% (95% CI, 1%-7%) and AKI was associated with in-hospital mortality of COVID-19 patients [91]. According to the latest treatment protocol (Pilot Version 7) issued by the Chinese Health Commission, continuous renal replacement therapy (CRRT) is recommended for patients with severe COVID-19 and renal damage, especially for those with stage 3 AKI. CRRT removes inflammatory cytokines to regulate renal metabolic adaptation and improves kidney energy balance to protect the kidneys in patients with AKI [92]. Wang et al. suggested that COVID-19 patients with renal dysfunction should be monitored regularly. Once acute kidney failure develops, potential interventions, including CRRT, should be immediately initiated to protect renal function [93]. However, CRRT intensity should be carefully determined. A study indicated that higher-intensity CRRT treatment did not reduce mortality in patients with severe COVID-19 and AKI as compared with that in the control group [94]. ...
Corticosteroid treatment of patients with coronavirus disease 2019 (COVID-19)
1
2020
... Corticosteroid treatment is a double-edged sword and its’ effectiveness in treating COVID-19 remains controversial. One study indicated that delayed viral clearance was not observed in patients treated with low dose corticosteroids, while another trial revealed that patients treated with a corticosteroid demonstrated more abnormalities on chest CT and more clinical symptoms [95, 96]. ARDS, the leading cause of death in patients with SARS and MERS, is also a challenge in COVID-19 patients. ARDS is closely associated with overwhelming inflammation and cytokine-related lung injury. A retrospective cohort study revealed that methylprednisolone treatment appears to reduce the risk of death in COVID-19 patients with ARDS (HR = 0.38; 95% CI, 0.20-0.72) [97]. Given the urgent clinical demand, corticosteroid treatment is weakly recommended for COVID-19 patients with ARDS due to the low-quality evidence. However, it is not recommended for routine treatment [98]. ...
Low-dose corticosteroid therapy does not delay viral clearance in patients with COVID-19
1
2020
... Corticosteroid treatment is a double-edged sword and its’ effectiveness in treating COVID-19 remains controversial. One study indicated that delayed viral clearance was not observed in patients treated with low dose corticosteroids, while another trial revealed that patients treated with a corticosteroid demonstrated more abnormalities on chest CT and more clinical symptoms [95, 96]. ARDS, the leading cause of death in patients with SARS and MERS, is also a challenge in COVID-19 patients. ARDS is closely associated with overwhelming inflammation and cytokine-related lung injury. A retrospective cohort study revealed that methylprednisolone treatment appears to reduce the risk of death in COVID-19 patients with ARDS (HR = 0.38; 95% CI, 0.20-0.72) [97]. Given the urgent clinical demand, corticosteroid treatment is weakly recommended for COVID-19 patients with ARDS due to the low-quality evidence. However, it is not recommended for routine treatment [98]. ...
Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China
1
2020
... Corticosteroid treatment is a double-edged sword and its’ effectiveness in treating COVID-19 remains controversial. One study indicated that delayed viral clearance was not observed in patients treated with low dose corticosteroids, while another trial revealed that patients treated with a corticosteroid demonstrated more abnormalities on chest CT and more clinical symptoms [95, 96]. ARDS, the leading cause of death in patients with SARS and MERS, is also a challenge in COVID-19 patients. ARDS is closely associated with overwhelming inflammation and cytokine-related lung injury. A retrospective cohort study revealed that methylprednisolone treatment appears to reduce the risk of death in COVID-19 patients with ARDS (HR = 0.38; 95% CI, 0.20-0.72) [97]. Given the urgent clinical demand, corticosteroid treatment is weakly recommended for COVID-19 patients with ARDS due to the low-quality evidence. However, it is not recommended for routine treatment [98]. ...
Management of Critically Ill Adults With COVID-19
1
2020
... Corticosteroid treatment is a double-edged sword and its’ effectiveness in treating COVID-19 remains controversial. One study indicated that delayed viral clearance was not observed in patients treated with low dose corticosteroids, while another trial revealed that patients treated with a corticosteroid demonstrated more abnormalities on chest CT and more clinical symptoms [95, 96]. ARDS, the leading cause of death in patients with SARS and MERS, is also a challenge in COVID-19 patients. ARDS is closely associated with overwhelming inflammation and cytokine-related lung injury. A retrospective cohort study revealed that methylprednisolone treatment appears to reduce the risk of death in COVID-19 patients with ARDS (HR = 0.38; 95% CI, 0.20-0.72) [97]. Given the urgent clinical demand, corticosteroid treatment is weakly recommended for COVID-19 patients with ARDS due to the low-quality evidence. However, it is not recommended for routine treatment [98]. ...
Role of lopinavir/ritonavir in the treatment of SARS: initial virological and clinical findings
1
2004
... One study found that SARS patients treated with LPV/r appeared to have a milder disease course, better outcomes, and significantly reduced viral loads [99]. Similarly, lopinavir has activity against MERS-CoV [100, 101]. As LPV/r is effective against other coronaviruses, researchers were optimistic to prescribe LPV/r for the treatment of COVID-19. However, a randomized, controlled, open-label trial conducted in China revealed that no significant difference was observed between LPV/r treatment and the control group of patients with severe COVID-19 in clinical improvement, reduced mortality, and/or changes in viral load [102]. The liver biopsy results of fatal COVID-19 patients indicated that the possibility of drug-induced acute liver injury could not be ruled out [103]. A study identified that patients with liver damage were administered a higher rate of LPV/r than that in those with normal liver function [104]. Hence, we do not recommend LPV/r as a routine treatment option for patients with a history of liver dysfunction. Further, clinicians should closely monitor liver-function indicators even in patients with normal liver function, if they are being treated with LPV/r. ...
Screening of an FDA-approved compound library identifies four small-molecule inhibitors of Middle East respiratory syndrome coronavirus replication in cell culture
1
2014
... One study found that SARS patients treated with LPV/r appeared to have a milder disease course, better outcomes, and significantly reduced viral loads [99]. Similarly, lopinavir has activity against MERS-CoV [100, 101]. As LPV/r is effective against other coronaviruses, researchers were optimistic to prescribe LPV/r for the treatment of COVID-19. However, a randomized, controlled, open-label trial conducted in China revealed that no significant difference was observed between LPV/r treatment and the control group of patients with severe COVID-19 in clinical improvement, reduced mortality, and/or changes in viral load [102]. The liver biopsy results of fatal COVID-19 patients indicated that the possibility of drug-induced acute liver injury could not be ruled out [103]. A study identified that patients with liver damage were administered a higher rate of LPV/r than that in those with normal liver function [104]. Hence, we do not recommend LPV/r as a routine treatment option for patients with a history of liver dysfunction. Further, clinicians should closely monitor liver-function indicators even in patients with normal liver function, if they are being treated with LPV/r. ...
Treatment With Lopinavir/Ritonavir or Interferon-beta1b Improves Outcome of MERS-CoV Infection in a Nonhuman Primate Model of Common Marmoset
1
2015
... One study found that SARS patients treated with LPV/r appeared to have a milder disease course, better outcomes, and significantly reduced viral loads [99]. Similarly, lopinavir has activity against MERS-CoV [100, 101]. As LPV/r is effective against other coronaviruses, researchers were optimistic to prescribe LPV/r for the treatment of COVID-19. However, a randomized, controlled, open-label trial conducted in China revealed that no significant difference was observed between LPV/r treatment and the control group of patients with severe COVID-19 in clinical improvement, reduced mortality, and/or changes in viral load [102]. The liver biopsy results of fatal COVID-19 patients indicated that the possibility of drug-induced acute liver injury could not be ruled out [103]. A study identified that patients with liver damage were administered a higher rate of LPV/r than that in those with normal liver function [104]. Hence, we do not recommend LPV/r as a routine treatment option for patients with a history of liver dysfunction. Further, clinicians should closely monitor liver-function indicators even in patients with normal liver function, if they are being treated with LPV/r. ...
A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe Covid-19
1
2020
... One study found that SARS patients treated with LPV/r appeared to have a milder disease course, better outcomes, and significantly reduced viral loads [99]. Similarly, lopinavir has activity against MERS-CoV [100, 101]. As LPV/r is effective against other coronaviruses, researchers were optimistic to prescribe LPV/r for the treatment of COVID-19. However, a randomized, controlled, open-label trial conducted in China revealed that no significant difference was observed between LPV/r treatment and the control group of patients with severe COVID-19 in clinical improvement, reduced mortality, and/or changes in viral load [102]. The liver biopsy results of fatal COVID-19 patients indicated that the possibility of drug-induced acute liver injury could not be ruled out [103]. A study identified that patients with liver damage were administered a higher rate of LPV/r than that in those with normal liver function [104]. Hence, we do not recommend LPV/r as a routine treatment option for patients with a history of liver dysfunction. Further, clinicians should closely monitor liver-function indicators even in patients with normal liver function, if they are being treated with LPV/r. ...
Pathological Study of the 2019 Novel Coronavirus Disease (COVID-19) through Post-Mortem Core Biopsies
5
2020
... One study found that SARS patients treated with LPV/r appeared to have a milder disease course, better outcomes, and significantly reduced viral loads [99]. Similarly, lopinavir has activity against MERS-CoV [100, 101]. As LPV/r is effective against other coronaviruses, researchers were optimistic to prescribe LPV/r for the treatment of COVID-19. However, a randomized, controlled, open-label trial conducted in China revealed that no significant difference was observed between LPV/r treatment and the control group of patients with severe COVID-19 in clinical improvement, reduced mortality, and/or changes in viral load [102]. The liver biopsy results of fatal COVID-19 patients indicated that the possibility of drug-induced acute liver injury could not be ruled out [103]. A study identified that patients with liver damage were administered a higher rate of LPV/r than that in those with normal liver function [104]. Hence, we do not recommend LPV/r as a routine treatment option for patients with a history of liver dysfunction. Further, clinicians should closely monitor liver-function indicators even in patients with normal liver function, if they are being treated with LPV/r. ...
... Another key finding is that COVID-19 appears to target multiple organs and induces acute injury. Li et al. found that the condition of patients without AKI at admission could gradually worsen and AKI may be diagnosed during hospitalization [147]. Guo et al. reported that some patients without underlying CVD had elevated TnT levels [148]. In this study, further analysis indicated that the incidence of acute multiorgan injury was considerably higher in patients with severe COVID-19. Similar to SARS-CoV, SARS-CoV-2 uses angiotensin-converting enzyme 2 (ACE2) as the cell entry receptor [149]. Zhao et al. demonstrated that ACE2 was principally expressed in alveolar epithelial type II cells, suggesting that the lung could be the most vulnerable target organ. However, ACE2 is highly expressed in the heart, kidney, liver, brain, and digestive tract, which provides a means for the involvement of multiple organs in COVID-19 [150-152]. Immunostaining of lung tissues indicated that the Rp3 nucleocapsid protein (NP) of SARS-CoV-2 was prominently expressed on alveolar epithelial cells, and histopathological examination revealed all the features of diffuse alveolar damage [103, 153]. Diao et al. found that various degrees of acute tubular necrosis and viral infection-associated syncytia were observed in renal specimens of COVID-19 patients. Furthermore, the NP antigens of SARS-CoV-2 could be observed in kidney tissues [154]. Clusters of coronavirus particles with distinctive spikes were observed in the tubular epithelium and podocytes [155]. No substantial histological changes were identified in the heart [103, 156], however SARS-CoV-2 viral particles have been identified in cardiac tissue in some COVID-19 cases [157, 158]. Biopsy of liver tissues revealed moderate microvesicular steatosis and mild lobular and portal activity; however, the possibility of drug-induced acute liver injury cannot be ruled out [103]. It has been reported that liver injury observed in COVID-19 patients after admission may be caused by LPV/r treatment [104]. Notably, viral RNA was also detected in the liver tissues of COVID-19 patients [158]. Similar to SARS-CoV, SARS-CoV-2 might invade the central nervous system via the nose close to the olfactory epithelium [159]. This was supported by the presence of olfactory disorders in patients with COVID-19. Detectable viral RNA was identified in the brain tissues of some COVID-19 cases [158], and the presence of specific SARS-CoV-2 RNA in COVID-19 patients’ cerebrospinal fluid has also been confirmed [160]. The SARS-CoV-2 RNA and NP were detected in GI tissues from COVID-19 patients [161]. In addition, the successful isolation of SARS-CoV-2 from stool samples demonstrated the fact that there was GI infection [162]. These results suggested that regional viral replication could directly contribute to acute organ damage. Of note, inflammatory cellular infiltration is commonly observed in multiple organs, including the lung, heart, kidney, and liver. This suggests that viruses not only induce direct organ damage but also aggravate the injury through proinflammatory function or cytokine storms [103, 156, 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection. ...
... ]. No substantial histological changes were identified in the heart [103, 156], however SARS-CoV-2 viral particles have been identified in cardiac tissue in some COVID-19 cases [157, 158]. Biopsy of liver tissues revealed moderate microvesicular steatosis and mild lobular and portal activity; however, the possibility of drug-induced acute liver injury cannot be ruled out [103]. It has been reported that liver injury observed in COVID-19 patients after admission may be caused by LPV/r treatment [104]. Notably, viral RNA was also detected in the liver tissues of COVID-19 patients [158]. Similar to SARS-CoV, SARS-CoV-2 might invade the central nervous system via the nose close to the olfactory epithelium [159]. This was supported by the presence of olfactory disorders in patients with COVID-19. Detectable viral RNA was identified in the brain tissues of some COVID-19 cases [158], and the presence of specific SARS-CoV-2 RNA in COVID-19 patients’ cerebrospinal fluid has also been confirmed [160]. The SARS-CoV-2 RNA and NP were detected in GI tissues from COVID-19 patients [161]. In addition, the successful isolation of SARS-CoV-2 from stool samples demonstrated the fact that there was GI infection [162]. These results suggested that regional viral replication could directly contribute to acute organ damage. Of note, inflammatory cellular infiltration is commonly observed in multiple organs, including the lung, heart, kidney, and liver. This suggests that viruses not only induce direct organ damage but also aggravate the injury through proinflammatory function or cytokine storms [103, 156, 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection. ...
... ]. Biopsy of liver tissues revealed moderate microvesicular steatosis and mild lobular and portal activity; however, the possibility of drug-induced acute liver injury cannot be ruled out [103]. It has been reported that liver injury observed in COVID-19 patients after admission may be caused by LPV/r treatment [104]. Notably, viral RNA was also detected in the liver tissues of COVID-19 patients [158]. Similar to SARS-CoV, SARS-CoV-2 might invade the central nervous system via the nose close to the olfactory epithelium [159]. This was supported by the presence of olfactory disorders in patients with COVID-19. Detectable viral RNA was identified in the brain tissues of some COVID-19 cases [158], and the presence of specific SARS-CoV-2 RNA in COVID-19 patients’ cerebrospinal fluid has also been confirmed [160]. The SARS-CoV-2 RNA and NP were detected in GI tissues from COVID-19 patients [161]. In addition, the successful isolation of SARS-CoV-2 from stool samples demonstrated the fact that there was GI infection [162]. These results suggested that regional viral replication could directly contribute to acute organ damage. Of note, inflammatory cellular infiltration is commonly observed in multiple organs, including the lung, heart, kidney, and liver. This suggests that viruses not only induce direct organ damage but also aggravate the injury through proinflammatory function or cytokine storms [103, 156, 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection. ...
... ]. These results suggested that regional viral replication could directly contribute to acute organ damage. Of note, inflammatory cellular infiltration is commonly observed in multiple organs, including the lung, heart, kidney, and liver. This suggests that viruses not only induce direct organ damage but also aggravate the injury through proinflammatory function or cytokine storms [103, 156, 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection. ...
Clinical Features of COVID-19-Related Liver Damage
2
2020
... One study found that SARS patients treated with LPV/r appeared to have a milder disease course, better outcomes, and significantly reduced viral loads [99]. Similarly, lopinavir has activity against MERS-CoV [100, 101]. As LPV/r is effective against other coronaviruses, researchers were optimistic to prescribe LPV/r for the treatment of COVID-19. However, a randomized, controlled, open-label trial conducted in China revealed that no significant difference was observed between LPV/r treatment and the control group of patients with severe COVID-19 in clinical improvement, reduced mortality, and/or changes in viral load [102]. The liver biopsy results of fatal COVID-19 patients indicated that the possibility of drug-induced acute liver injury could not be ruled out [103]. A study identified that patients with liver damage were administered a higher rate of LPV/r than that in those with normal liver function [104]. Hence, we do not recommend LPV/r as a routine treatment option for patients with a history of liver dysfunction. Further, clinicians should closely monitor liver-function indicators even in patients with normal liver function, if they are being treated with LPV/r. ...
... Another key finding is that COVID-19 appears to target multiple organs and induces acute injury. Li et al. found that the condition of patients without AKI at admission could gradually worsen and AKI may be diagnosed during hospitalization [147]. Guo et al. reported that some patients without underlying CVD had elevated TnT levels [148]. In this study, further analysis indicated that the incidence of acute multiorgan injury was considerably higher in patients with severe COVID-19. Similar to SARS-CoV, SARS-CoV-2 uses angiotensin-converting enzyme 2 (ACE2) as the cell entry receptor [149]. Zhao et al. demonstrated that ACE2 was principally expressed in alveolar epithelial type II cells, suggesting that the lung could be the most vulnerable target organ. However, ACE2 is highly expressed in the heart, kidney, liver, brain, and digestive tract, which provides a means for the involvement of multiple organs in COVID-19 [150-152]. Immunostaining of lung tissues indicated that the Rp3 nucleocapsid protein (NP) of SARS-CoV-2 was prominently expressed on alveolar epithelial cells, and histopathological examination revealed all the features of diffuse alveolar damage [103, 153]. Diao et al. found that various degrees of acute tubular necrosis and viral infection-associated syncytia were observed in renal specimens of COVID-19 patients. Furthermore, the NP antigens of SARS-CoV-2 could be observed in kidney tissues [154]. Clusters of coronavirus particles with distinctive spikes were observed in the tubular epithelium and podocytes [155]. No substantial histological changes were identified in the heart [103, 156], however SARS-CoV-2 viral particles have been identified in cardiac tissue in some COVID-19 cases [157, 158]. Biopsy of liver tissues revealed moderate microvesicular steatosis and mild lobular and portal activity; however, the possibility of drug-induced acute liver injury cannot be ruled out [103]. It has been reported that liver injury observed in COVID-19 patients after admission may be caused by LPV/r treatment [104]. Notably, viral RNA was also detected in the liver tissues of COVID-19 patients [158]. Similar to SARS-CoV, SARS-CoV-2 might invade the central nervous system via the nose close to the olfactory epithelium [159]. This was supported by the presence of olfactory disorders in patients with COVID-19. Detectable viral RNA was identified in the brain tissues of some COVID-19 cases [158], and the presence of specific SARS-CoV-2 RNA in COVID-19 patients’ cerebrospinal fluid has also been confirmed [160]. The SARS-CoV-2 RNA and NP were detected in GI tissues from COVID-19 patients [161]. In addition, the successful isolation of SARS-CoV-2 from stool samples demonstrated the fact that there was GI infection [162]. These results suggested that regional viral replication could directly contribute to acute organ damage. Of note, inflammatory cellular infiltration is commonly observed in multiple organs, including the lung, heart, kidney, and liver. This suggests that viruses not only induce direct organ damage but also aggravate the injury through proinflammatory function or cytokine storms [103, 156, 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection. ...
Characteristics of ischaemic stroke associated with COVID-19
1
2020
... Ischemic stroke has been recognized as a complication in patients with COVID-19, especially in patients with severe infection [105]. However, the precise mechanisms are not yet clear. Obviously, an elevated D-dimer level was noted in patients with COVID-19 who developed stroke, indicating a hypercoagulable state [106]. It was suggested that production of antiphospholipid antibodies (aPL) accompanying COVID-19 infection may be closely associated with both venous and arterial thrombotic events [107]. The mortality of COVID-19 patients with stroke was much higher than that of patients with stroke alone [106, 108]. Considering the high mortality and prothrombotic state, it seems reasonable to initiate treatment with anticoagulants such as low molecular weight heparin (LMWH) and a recombinant tissue plasminogen activator (rt-PA) [109]. Compared with antiplatelet treatment, patients treated with LMWH had lower mortality [106]. Notably, patients who developed stroke were more likely to have multiple organ dysfunction [106]. Patients with hepatic dysfunction may have a significant reduction in their ability of hepatic clearance, which would increase the risk of intracranial hemorrhage (ICH). In addition, leukocytosis, elevated C reactive protein levels and D-dimer, which were commonly seen in COVID-19 patients, were identified as risk factors of ICH among patients without COVID-19 infection [110]. Therefore, it is reasonable to assess the coagulation profile for COVID-19 patients with acute ischemic stroke prior to administration of rt-PA and LMWH to determine the risk benefit ratio [109]. ...
Acute Cerebrovascular Disease Following COVID-19: A Single Center, Retrospective, Observational Study
4
2020
... Ischemic stroke has been recognized as a complication in patients with COVID-19, especially in patients with severe infection [105]. However, the precise mechanisms are not yet clear. Obviously, an elevated D-dimer level was noted in patients with COVID-19 who developed stroke, indicating a hypercoagulable state [106]. It was suggested that production of antiphospholipid antibodies (aPL) accompanying COVID-19 infection may be closely associated with both venous and arterial thrombotic events [107]. The mortality of COVID-19 patients with stroke was much higher than that of patients with stroke alone [106, 108]. Considering the high mortality and prothrombotic state, it seems reasonable to initiate treatment with anticoagulants such as low molecular weight heparin (LMWH) and a recombinant tissue plasminogen activator (rt-PA) [109]. Compared with antiplatelet treatment, patients treated with LMWH had lower mortality [106]. Notably, patients who developed stroke were more likely to have multiple organ dysfunction [106]. Patients with hepatic dysfunction may have a significant reduction in their ability of hepatic clearance, which would increase the risk of intracranial hemorrhage (ICH). In addition, leukocytosis, elevated C reactive protein levels and D-dimer, which were commonly seen in COVID-19 patients, were identified as risk factors of ICH among patients without COVID-19 infection [110]. Therefore, it is reasonable to assess the coagulation profile for COVID-19 patients with acute ischemic stroke prior to administration of rt-PA and LMWH to determine the risk benefit ratio [109]. ...
... ]. The mortality of COVID-19 patients with stroke was much higher than that of patients with stroke alone [106, 108]. Considering the high mortality and prothrombotic state, it seems reasonable to initiate treatment with anticoagulants such as low molecular weight heparin (LMWH) and a recombinant tissue plasminogen activator (rt-PA) [109]. Compared with antiplatelet treatment, patients treated with LMWH had lower mortality [106]. Notably, patients who developed stroke were more likely to have multiple organ dysfunction [106]. Patients with hepatic dysfunction may have a significant reduction in their ability of hepatic clearance, which would increase the risk of intracranial hemorrhage (ICH). In addition, leukocytosis, elevated C reactive protein levels and D-dimer, which were commonly seen in COVID-19 patients, were identified as risk factors of ICH among patients without COVID-19 infection [110]. Therefore, it is reasonable to assess the coagulation profile for COVID-19 patients with acute ischemic stroke prior to administration of rt-PA and LMWH to determine the risk benefit ratio [109]. ...
... ]. Compared with antiplatelet treatment, patients treated with LMWH had lower mortality [106]. Notably, patients who developed stroke were more likely to have multiple organ dysfunction [106]. Patients with hepatic dysfunction may have a significant reduction in their ability of hepatic clearance, which would increase the risk of intracranial hemorrhage (ICH). In addition, leukocytosis, elevated C reactive protein levels and D-dimer, which were commonly seen in COVID-19 patients, were identified as risk factors of ICH among patients without COVID-19 infection [110]. Therefore, it is reasonable to assess the coagulation profile for COVID-19 patients with acute ischemic stroke prior to administration of rt-PA and LMWH to determine the risk benefit ratio [109]. ...
... ]. Notably, patients who developed stroke were more likely to have multiple organ dysfunction [106]. Patients with hepatic dysfunction may have a significant reduction in their ability of hepatic clearance, which would increase the risk of intracranial hemorrhage (ICH). In addition, leukocytosis, elevated C reactive protein levels and D-dimer, which were commonly seen in COVID-19 patients, were identified as risk factors of ICH among patients without COVID-19 infection [110]. Therefore, it is reasonable to assess the coagulation profile for COVID-19 patients with acute ischemic stroke prior to administration of rt-PA and LMWH to determine the risk benefit ratio [109]. ...
Coagulopathy and Antiphospholipid Antibodies in Patients with Covid-19
1
2020
... Ischemic stroke has been recognized as a complication in patients with COVID-19, especially in patients with severe infection [105]. However, the precise mechanisms are not yet clear. Obviously, an elevated D-dimer level was noted in patients with COVID-19 who developed stroke, indicating a hypercoagulable state [106]. It was suggested that production of antiphospholipid antibodies (aPL) accompanying COVID-19 infection may be closely associated with both venous and arterial thrombotic events [107]. The mortality of COVID-19 patients with stroke was much higher than that of patients with stroke alone [106, 108]. Considering the high mortality and prothrombotic state, it seems reasonable to initiate treatment with anticoagulants such as low molecular weight heparin (LMWH) and a recombinant tissue plasminogen activator (rt-PA) [109]. Compared with antiplatelet treatment, patients treated with LMWH had lower mortality [106]. Notably, patients who developed stroke were more likely to have multiple organ dysfunction [106]. Patients with hepatic dysfunction may have a significant reduction in their ability of hepatic clearance, which would increase the risk of intracranial hemorrhage (ICH). In addition, leukocytosis, elevated C reactive protein levels and D-dimer, which were commonly seen in COVID-19 patients, were identified as risk factors of ICH among patients without COVID-19 infection [110]. Therefore, it is reasonable to assess the coagulation profile for COVID-19 patients with acute ischemic stroke prior to administration of rt-PA and LMWH to determine the risk benefit ratio [109]. ...
Trends in in-hospital mortality among patients with stroke in China
1
2014
... Ischemic stroke has been recognized as a complication in patients with COVID-19, especially in patients with severe infection [105]. However, the precise mechanisms are not yet clear. Obviously, an elevated D-dimer level was noted in patients with COVID-19 who developed stroke, indicating a hypercoagulable state [106]. It was suggested that production of antiphospholipid antibodies (aPL) accompanying COVID-19 infection may be closely associated with both venous and arterial thrombotic events [107]. The mortality of COVID-19 patients with stroke was much higher than that of patients with stroke alone [106, 108]. Considering the high mortality and prothrombotic state, it seems reasonable to initiate treatment with anticoagulants such as low molecular weight heparin (LMWH) and a recombinant tissue plasminogen activator (rt-PA) [109]. Compared with antiplatelet treatment, patients treated with LMWH had lower mortality [106]. Notably, patients who developed stroke were more likely to have multiple organ dysfunction [106]. Patients with hepatic dysfunction may have a significant reduction in their ability of hepatic clearance, which would increase the risk of intracranial hemorrhage (ICH). In addition, leukocytosis, elevated C reactive protein levels and D-dimer, which were commonly seen in COVID-19 patients, were identified as risk factors of ICH among patients without COVID-19 infection [110]. Therefore, it is reasonable to assess the coagulation profile for COVID-19 patients with acute ischemic stroke prior to administration of rt-PA and LMWH to determine the risk benefit ratio [109]. ...
Management of acute ischemic stroke in patients with COVID-19 infection: Report of an international panel
2
2020
... Ischemic stroke has been recognized as a complication in patients with COVID-19, especially in patients with severe infection [105]. However, the precise mechanisms are not yet clear. Obviously, an elevated D-dimer level was noted in patients with COVID-19 who developed stroke, indicating a hypercoagulable state [106]. It was suggested that production of antiphospholipid antibodies (aPL) accompanying COVID-19 infection may be closely associated with both venous and arterial thrombotic events [107]. The mortality of COVID-19 patients with stroke was much higher than that of patients with stroke alone [106, 108]. Considering the high mortality and prothrombotic state, it seems reasonable to initiate treatment with anticoagulants such as low molecular weight heparin (LMWH) and a recombinant tissue plasminogen activator (rt-PA) [109]. Compared with antiplatelet treatment, patients treated with LMWH had lower mortality [106]. Notably, patients who developed stroke were more likely to have multiple organ dysfunction [106]. Patients with hepatic dysfunction may have a significant reduction in their ability of hepatic clearance, which would increase the risk of intracranial hemorrhage (ICH). In addition, leukocytosis, elevated C reactive protein levels and D-dimer, which were commonly seen in COVID-19 patients, were identified as risk factors of ICH among patients without COVID-19 infection [110]. Therefore, it is reasonable to assess the coagulation profile for COVID-19 patients with acute ischemic stroke prior to administration of rt-PA and LMWH to determine the risk benefit ratio [109]. ...
... ]. Therefore, it is reasonable to assess the coagulation profile for COVID-19 patients with acute ischemic stroke prior to administration of rt-PA and LMWH to determine the risk benefit ratio [109]. ...
Body temperature, blood infection parameters, and outcome of thrombolysis-treated ischemic stroke patients
1
2013
... Ischemic stroke has been recognized as a complication in patients with COVID-19, especially in patients with severe infection [105]. However, the precise mechanisms are not yet clear. Obviously, an elevated D-dimer level was noted in patients with COVID-19 who developed stroke, indicating a hypercoagulable state [106]. It was suggested that production of antiphospholipid antibodies (aPL) accompanying COVID-19 infection may be closely associated with both venous and arterial thrombotic events [107]. The mortality of COVID-19 patients with stroke was much higher than that of patients with stroke alone [106, 108]. Considering the high mortality and prothrombotic state, it seems reasonable to initiate treatment with anticoagulants such as low molecular weight heparin (LMWH) and a recombinant tissue plasminogen activator (rt-PA) [109]. Compared with antiplatelet treatment, patients treated with LMWH had lower mortality [106]. Notably, patients who developed stroke were more likely to have multiple organ dysfunction [106]. Patients with hepatic dysfunction may have a significant reduction in their ability of hepatic clearance, which would increase the risk of intracranial hemorrhage (ICH). In addition, leukocytosis, elevated C reactive protein levels and D-dimer, which were commonly seen in COVID-19 patients, were identified as risk factors of ICH among patients without COVID-19 infection [110]. Therefore, it is reasonable to assess the coagulation profile for COVID-19 patients with acute ischemic stroke prior to administration of rt-PA and LMWH to determine the risk benefit ratio [109]. ...
Implications of COVID-19 for patients with pre-existing digestive diseases
2
2020
... As the COVID-19 pandemic expands, the impact of COVID-19 on patients with inflammatory bowel disease (IBD) has been a major concern. A significant number of IBD patients require immunosuppressors that target extensive inflammation. This may weaken the immune system and predispose IBD patients to a higher risk of COVID-19 infection. However, according to evidence emerging from China, Italy and other counties, there was no obvious indication that IBD patients were at greater risk of COVID-19 infection compared to the general population [111-113]. Thiopurines were related to a risk of serious viral infection in IBD patients, while a meta-analysis revealed that anti-tumor necrosis factor therapy was associated developing an opportunistic infection [114, 115]. However, discontinuation of IBD drugs should not be recommended for IBD patients during the COVID-19 pandemic [111]. This was supported by the results of the first case series report of COVID-19 infection in IBD patients [116]. Clinicians should be alert regarding patients treated with immunosuppressors and carefully monitor the presence of symptoms associated with COVID-19 [117]. The withholding of ongoing therapies should be considered only in confirmed COVID-19 patients. Therapies must be assessed carefully according to the balance between the severity of COVID-19 and the status of IBD [118]. ...
... ]. However, discontinuation of IBD drugs should not be recommended for IBD patients during the COVID-19 pandemic [111]. This was supported by the results of the first case series report of COVID-19 infection in IBD patients [116]. Clinicians should be alert regarding patients treated with immunosuppressors and carefully monitor the presence of symptoms associated with COVID-19 [117]. The withholding of ongoing therapies should be considered only in confirmed COVID-19 patients. Therapies must be assessed carefully according to the balance between the severity of COVID-19 and the status of IBD [118]. ...
Uneventful course in IBD patients during SARS-CoV-2 outbreak in northern Italy
0
2020
A fatal case of COVID-19 pneumonia occurring in a patient with severe acute ulcerative colitis
1
2020
... As the COVID-19 pandemic expands, the impact of COVID-19 on patients with inflammatory bowel disease (IBD) has been a major concern. A significant number of IBD patients require immunosuppressors that target extensive inflammation. This may weaken the immune system and predispose IBD patients to a higher risk of COVID-19 infection. However, according to evidence emerging from China, Italy and other counties, there was no obvious indication that IBD patients were at greater risk of COVID-19 infection compared to the general population [111-113]. Thiopurines were related to a risk of serious viral infection in IBD patients, while a meta-analysis revealed that anti-tumor necrosis factor therapy was associated developing an opportunistic infection [114, 115]. However, discontinuation of IBD drugs should not be recommended for IBD patients during the COVID-19 pandemic [111]. This was supported by the results of the first case series report of COVID-19 infection in IBD patients [116]. Clinicians should be alert regarding patients treated with immunosuppressors and carefully monitor the presence of symptoms associated with COVID-19 [117]. The withholding of ongoing therapies should be considered only in confirmed COVID-19 patients. Therapies must be assessed carefully according to the balance between the severity of COVID-19 and the status of IBD [118]. ...
Increased incidence of systemic serious viral infections in patients with inflammatory bowel disease associates with active disease and use of thiopurines
1
2020
... As the COVID-19 pandemic expands, the impact of COVID-19 on patients with inflammatory bowel disease (IBD) has been a major concern. A significant number of IBD patients require immunosuppressors that target extensive inflammation. This may weaken the immune system and predispose IBD patients to a higher risk of COVID-19 infection. However, according to evidence emerging from China, Italy and other counties, there was no obvious indication that IBD patients were at greater risk of COVID-19 infection compared to the general population [111-113]. Thiopurines were related to a risk of serious viral infection in IBD patients, while a meta-analysis revealed that anti-tumor necrosis factor therapy was associated developing an opportunistic infection [114, 115]. However, discontinuation of IBD drugs should not be recommended for IBD patients during the COVID-19 pandemic [111]. This was supported by the results of the first case series report of COVID-19 infection in IBD patients [116]. Clinicians should be alert regarding patients treated with immunosuppressors and carefully monitor the presence of symptoms associated with COVID-19 [117]. The withholding of ongoing therapies should be considered only in confirmed COVID-19 patients. Therapies must be assessed carefully according to the balance between the severity of COVID-19 and the status of IBD [118]. ...
Opportunistic infections with anti-tumor necrosis factor-alpha therapy in inflammatory bowel disease: meta-analysis of randomized controlled trials
1
2013
... As the COVID-19 pandemic expands, the impact of COVID-19 on patients with inflammatory bowel disease (IBD) has been a major concern. A significant number of IBD patients require immunosuppressors that target extensive inflammation. This may weaken the immune system and predispose IBD patients to a higher risk of COVID-19 infection. However, according to evidence emerging from China, Italy and other counties, there was no obvious indication that IBD patients were at greater risk of COVID-19 infection compared to the general population [111-113]. Thiopurines were related to a risk of serious viral infection in IBD patients, while a meta-analysis revealed that anti-tumor necrosis factor therapy was associated developing an opportunistic infection [114, 115]. However, discontinuation of IBD drugs should not be recommended for IBD patients during the COVID-19 pandemic [111]. This was supported by the results of the first case series report of COVID-19 infection in IBD patients [116]. Clinicians should be alert regarding patients treated with immunosuppressors and carefully monitor the presence of symptoms associated with COVID-19 [117]. The withholding of ongoing therapies should be considered only in confirmed COVID-19 patients. Therapies must be assessed carefully according to the balance between the severity of COVID-19 and the status of IBD [118]. ...
2019 Novel Coronavirus Disease (COVID-19) in patients with Inflammatory Bowel Diseases
1
2020
... As the COVID-19 pandemic expands, the impact of COVID-19 on patients with inflammatory bowel disease (IBD) has been a major concern. A significant number of IBD patients require immunosuppressors that target extensive inflammation. This may weaken the immune system and predispose IBD patients to a higher risk of COVID-19 infection. However, according to evidence emerging from China, Italy and other counties, there was no obvious indication that IBD patients were at greater risk of COVID-19 infection compared to the general population [111-113]. Thiopurines were related to a risk of serious viral infection in IBD patients, while a meta-analysis revealed that anti-tumor necrosis factor therapy was associated developing an opportunistic infection [114, 115]. However, discontinuation of IBD drugs should not be recommended for IBD patients during the COVID-19 pandemic [111]. This was supported by the results of the first case series report of COVID-19 infection in IBD patients [116]. Clinicians should be alert regarding patients treated with immunosuppressors and carefully monitor the presence of symptoms associated with COVID-19 [117]. The withholding of ongoing therapies should be considered only in confirmed COVID-19 patients. Therapies must be assessed carefully according to the balance between the severity of COVID-19 and the status of IBD [118]. ...
Are patients with inflammatory bowel disease at increased risk for Covid-19 infection?
1
2020
... As the COVID-19 pandemic expands, the impact of COVID-19 on patients with inflammatory bowel disease (IBD) has been a major concern. A significant number of IBD patients require immunosuppressors that target extensive inflammation. This may weaken the immune system and predispose IBD patients to a higher risk of COVID-19 infection. However, according to evidence emerging from China, Italy and other counties, there was no obvious indication that IBD patients were at greater risk of COVID-19 infection compared to the general population [111-113]. Thiopurines were related to a risk of serious viral infection in IBD patients, while a meta-analysis revealed that anti-tumor necrosis factor therapy was associated developing an opportunistic infection [114, 115]. However, discontinuation of IBD drugs should not be recommended for IBD patients during the COVID-19 pandemic [111]. This was supported by the results of the first case series report of COVID-19 infection in IBD patients [116]. Clinicians should be alert regarding patients treated with immunosuppressors and carefully monitor the presence of symptoms associated with COVID-19 [117]. The withholding of ongoing therapies should be considered only in confirmed COVID-19 patients. Therapies must be assessed carefully according to the balance between the severity of COVID-19 and the status of IBD [118]. ...
Inflammatory Bowel Diseases and COVID-19: The Invisible Enemy
1
2020
... As the COVID-19 pandemic expands, the impact of COVID-19 on patients with inflammatory bowel disease (IBD) has been a major concern. A significant number of IBD patients require immunosuppressors that target extensive inflammation. This may weaken the immune system and predispose IBD patients to a higher risk of COVID-19 infection. However, according to evidence emerging from China, Italy and other counties, there was no obvious indication that IBD patients were at greater risk of COVID-19 infection compared to the general population [111-113]. Thiopurines were related to a risk of serious viral infection in IBD patients, while a meta-analysis revealed that anti-tumor necrosis factor therapy was associated developing an opportunistic infection [114, 115]. However, discontinuation of IBD drugs should not be recommended for IBD patients during the COVID-19 pandemic [111]. This was supported by the results of the first case series report of COVID-19 infection in IBD patients [116]. Clinicians should be alert regarding patients treated with immunosuppressors and carefully monitor the presence of symptoms associated with COVID-19 [117]. The withholding of ongoing therapies should be considered only in confirmed COVID-19 patients. Therapies must be assessed carefully according to the balance between the severity of COVID-19 and the status of IBD [118]. ...
Prognostic factors for severe acute respiratory syndrome: a clinical analysis of 165 cases
1
2004
... We searched related articles to undertake a meta-analysis of SARS and MERS. The strategies were similar to COVID-19 [119-137]. ...
Outcomes and prognostic factors in 267 patients with severe acute respiratory syndrome in Hong Kong
0
2003
Correlation of clinical outcomes and radiographic features in SARS patients
0
2009
Acute respiratory distress syndrome in critically ill patients with severe acute respiratory syndrome
0
2003
Prognostication in severe acute respiratory syndrome: a retrospective time-course analysis of 1312 laboratory-confirmed patients in Hong Kong
1
2007
... CVD is a risk factor for predicting the severity of COVID-19, MERS, and SARS [138]. Similar to COVID-19 patients, LDH (WMD = 124.14 U/L; 95% CI, 31.09-217.19 U/L) and CK (WMD = 149.91 U/L; 95% CI, 94.03-205.79 U/L) levels of patients with severe SARS are frequently high. However, few studies have compared LDH and CK levels in patients with severe and non-severe MERS. As presented in Table 2, patients with either of the three viruses and renal and pulmonary dysfunction on admission were at high risk of developing severe disease. CLD was also a risk factor for the severity of SARS and MERS. No significant differences in ALT levels (WMD = -3.07 U/L; 95% CI, -11.26-5.11 U/L) or AST levels (WMD = 34.81 U/L; 95% CI, -4.39-74.02 U/L) was observed between patients with severe MERS and non-severe MERS (Table 2). Limited studies reported the relationship between neurologic dysfunction or GI dysfunction and SARS or MERS severity. Unlike SARS (P<0.001); [123] and COVID-19, chronic cerebrovascular diseases was not a predictor for the severity of MERS (OR = 1.94; 95% CI, 0.69-5.43); (Supplementary Fig. 2-6). ...
Severe acute respiratory syndrome in Taiwan: analysis of epidemiological characteristics in 29 cases
0
2004
Clinical features and short-term outcomes of 144 patients with SARS in the greater Toronto area
0
2003
A major outbreak of severe acute respiratory syndrome in Hong Kong
0
2003
Clinical progression and viral load in a community outbreak of coronavirus-associated SARS pneumonia: a prospective study
0
2003
Cardiovascular complications of severe acute respiratory syndrome
0
2006
Critically ill patients with severe acute respiratory syndrome
0
2003
Clinical predictors of mortality of Middle East Respiratory Syndrome Coronavirus (MERS-CoV) infection: A cohort study
0
2019
Critically Ill Patients With the Middle East Respiratory Syndrome: A Multicenter Retrospective Cohort Study
0
2017
Middle East respiratory syndrome coronavirus in Al-Madinah City, Saudi Arabia: Demographic, clinical and survival data
0
2017
Clinical Presentation and Outcomes of Middle East Respiratory Syndrome in the Republic of Korea
0
2016
Multifacility Outbreak of Middle East Respiratory Syndrome in Taif, Saudi Arabia
0
2016
Presentation and outcome of Middle East respiratory syndrome in Saudi intensive care unit patients
0
2016
Prevalence of comorbidities in cases of Middle East respiratory syndrome coronavirus: a retrospective study
0
2018
Value of initial chest radiographs for predicting clinical outcomes in patients with severe acute respiratory syndrome
1
2004
... We searched related articles to undertake a meta-analysis of SARS and MERS. The strategies were similar to COVID-19 [119-137]. ...
Clinical determinants of the severity of Middle East respiratory syndrome (MERS): a systematic review and meta-analysis
1
2016
... CVD is a risk factor for predicting the severity of COVID-19, MERS, and SARS [138]. Similar to COVID-19 patients, LDH (WMD = 124.14 U/L; 95% CI, 31.09-217.19 U/L) and CK (WMD = 149.91 U/L; 95% CI, 94.03-205.79 U/L) levels of patients with severe SARS are frequently high. However, few studies have compared LDH and CK levels in patients with severe and non-severe MERS. As presented in Table 2, patients with either of the three viruses and renal and pulmonary dysfunction on admission were at high risk of developing severe disease. CLD was also a risk factor for the severity of SARS and MERS. No significant differences in ALT levels (WMD = -3.07 U/L; 95% CI, -11.26-5.11 U/L) or AST levels (WMD = 34.81 U/L; 95% CI, -4.39-74.02 U/L) was observed between patients with severe MERS and non-severe MERS (Table 2). Limited studies reported the relationship between neurologic dysfunction or GI dysfunction and SARS or MERS severity. Unlike SARS (P<0.001); [123] and COVID-19, chronic cerebrovascular diseases was not a predictor for the severity of MERS (OR = 1.94; 95% CI, 0.69-5.43); (Supplementary Fig. 2-6). ...
Chronic obstructive pulmonary disease in China: a nationwide prevalence study
1
2018
... According to studies on COVID-19, the presence of comorbidities is a predictor of a poor outcome. It is important to evaluate the prevalence of comorbidities in COVID-19 patients. In the present meta-analysis, the overall proportion of patients with hypertension, diabetes, CVD, chronic GI diseases, chronic cerebrovascular diseases, COPD, CLD, and CKD was 19%, 10%, 8%, 7%, 3%, 2%, 3%, and 3%, respectively. However, the prevalence of these chronic diseases is considerably higher in the general population [139, 140]. Hence, we could not determine whether patients with comorbidities are more susceptible to COVID-19 infection. ...
Status of Hypertension in China: Results From the China Hypertension Survey, 2012-2015
1
2018
... According to studies on COVID-19, the presence of comorbidities is a predictor of a poor outcome. It is important to evaluate the prevalence of comorbidities in COVID-19 patients. In the present meta-analysis, the overall proportion of patients with hypertension, diabetes, CVD, chronic GI diseases, chronic cerebrovascular diseases, COPD, CLD, and CKD was 19%, 10%, 8%, 7%, 3%, 2%, 3%, and 3%, respectively. However, the prevalence of these chronic diseases is considerably higher in the general population [139, 140]. Hence, we could not determine whether patients with comorbidities are more susceptible to COVID-19 infection. ...
Incidence, clinical characteristics and prognostic factor of patients with COVID-19: a systematic review and meta-analysis
2
2020
... However, we assuredly do know that patients with comorbidities such as hypertension, CVD, CKD and COPD, are vulnerable to developing severe disease, which is consistent with previous studies [7, 141]. It can be speculated that comorbidities influence COVID-19 through two mechanisms. First, comorbidities are more prevalent among individuals of advanced age. Innate immunity serves as the first line of defense against pathogen invasion, and successful mounting of type I interferon (IFN) response should be able to suppress viral replication at an early stage [142]. Aging has been reported to impair the capacity of plasmacytoid dendritic cells, which are the most important type of I IFN producing cells [143, 144]. When the innate immune response is not effective and a delayed-type I IFN response is mounted, the virus cannot be controlled in the early phase of infection and patients are more likely to develop a severe infection. Second, in SARS and MERS infection, the influx of hyperinflammatory cytokines and chemokines is the main cause of lethal outcomes [144, 145]. Huang et al. reported that in COVID-19, higher levels of inflammatory factors were more commonly seen in patients with severe COVID-19 than in those with non-severe COVID-19, suggesting that a cytokine storm was associated with disease severity [8]. Patients with various chronic diseases are already in a proinflammatory state with impaired immune function; hence, the infection can accelerate the inflammatory progress [146]. Therefore, patients with a history of organ dysfunction may have a greater risk of developing severe COVID-19. ...
... SARS-CoV, MERS-CoV, and SARS-CoV-2 belong to the same genus and all are beta-CoVs. The comparison of genomic sequences revealed that the SARS-CoV-2 genome is 79% and 50% similar to SARS-CoV and MERS-CoV, respectively. SARS-CoV-2 contains additional gene regions, and the amino acid sequences of some SARS-CoV-2 proteins are only 68% similar to those of SARS-CoV [144, 163, 164]. It is reasonable to speculate that SARS-CoV-2 has similar clinical features and pathology as SARS-CoV and MERS-CoV; however, additional characteristics may yet be discovered. These findings reveal that all three coronaviruses might originate in bats prior to mutations. Subsequently they adapt to intermediate hosts and finally to humans [163, 165]. SARS-CoV and SARS-CoV-2 share the cell entry receptor of ACE2, while Dipeptidyl peptidase (DPP)-4 serves as the specific receptor for MERS-CoV [144, 166]. Similar to SARS and MERS, lower respiratory symptoms, including fever, cough, and fatigue, were commonly observed in patients with early-stage COVID-19, while the incidence of GI symptoms was relatively low [17, 141]. In the present study, a history of organ dysfunction was identified as the predictor of severe disease in all three coronaviruses. In addition, the pathological changes in the multiorgan tissues of COVID-19 patients significantly resemble those observed in SARS and MERS infection. This provides evidence for our work [167, 168]. Coronaviruses not only induce direct organ damage but also aggravate the injury through proinflammatory methods. On the basis of the information from previous studies, we found that SARS-CoV-2 shared similarities with SARS-CoV and/or MERS-CoV in various aspects, including genomic sequence, origin, entry receptor, clinical features, risk factors, and pathological processes. As no vaccine or specific treatment with confirmed results is available for treating COVID-19, and COVID-19 has a huge impact, clinical experience from SARS and MERS may provide some guidance regarding treatment strategies that may benefit COVID-19 patients. ...
SARS and MERS: recent insights into emerging coronaviruses
1
2016
... However, we assuredly do know that patients with comorbidities such as hypertension, CVD, CKD and COPD, are vulnerable to developing severe disease, which is consistent with previous studies [7, 141]. It can be speculated that comorbidities influence COVID-19 through two mechanisms. First, comorbidities are more prevalent among individuals of advanced age. Innate immunity serves as the first line of defense against pathogen invasion, and successful mounting of type I interferon (IFN) response should be able to suppress viral replication at an early stage [142]. Aging has been reported to impair the capacity of plasmacytoid dendritic cells, which are the most important type of I IFN producing cells [143, 144]. When the innate immune response is not effective and a delayed-type I IFN response is mounted, the virus cannot be controlled in the early phase of infection and patients are more likely to develop a severe infection. Second, in SARS and MERS infection, the influx of hyperinflammatory cytokines and chemokines is the main cause of lethal outcomes [144, 145]. Huang et al. reported that in COVID-19, higher levels of inflammatory factors were more commonly seen in patients with severe COVID-19 than in those with non-severe COVID-19, suggesting that a cytokine storm was associated with disease severity [8]. Patients with various chronic diseases are already in a proinflammatory state with impaired immune function; hence, the infection can accelerate the inflammatory progress [146]. Therefore, patients with a history of organ dysfunction may have a greater risk of developing severe COVID-19. ...
Plasmacytoid dendritic cells: key players in the initiation and regulation of immune responses
1
2010
... However, we assuredly do know that patients with comorbidities such as hypertension, CVD, CKD and COPD, are vulnerable to developing severe disease, which is consistent with previous studies [7, 141]. It can be speculated that comorbidities influence COVID-19 through two mechanisms. First, comorbidities are more prevalent among individuals of advanced age. Innate immunity serves as the first line of defense against pathogen invasion, and successful mounting of type I interferon (IFN) response should be able to suppress viral replication at an early stage [142]. Aging has been reported to impair the capacity of plasmacytoid dendritic cells, which are the most important type of I IFN producing cells [143, 144]. When the innate immune response is not effective and a delayed-type I IFN response is mounted, the virus cannot be controlled in the early phase of infection and patients are more likely to develop a severe infection. Second, in SARS and MERS infection, the influx of hyperinflammatory cytokines and chemokines is the main cause of lethal outcomes [144, 145]. Huang et al. reported that in COVID-19, higher levels of inflammatory factors were more commonly seen in patients with severe COVID-19 than in those with non-severe COVID-19, suggesting that a cytokine storm was associated with disease severity [8]. Patients with various chronic diseases are already in a proinflammatory state with impaired immune function; hence, the infection can accelerate the inflammatory progress [146]. Therefore, patients with a history of organ dysfunction may have a greater risk of developing severe COVID-19. ...
Immune responses in COVID-19 and potential vaccines: Lessons learned from SARS and MERS epidemic
4
2020
... However, we assuredly do know that patients with comorbidities such as hypertension, CVD, CKD and COPD, are vulnerable to developing severe disease, which is consistent with previous studies [7, 141]. It can be speculated that comorbidities influence COVID-19 through two mechanisms. First, comorbidities are more prevalent among individuals of advanced age. Innate immunity serves as the first line of defense against pathogen invasion, and successful mounting of type I interferon (IFN) response should be able to suppress viral replication at an early stage [142]. Aging has been reported to impair the capacity of plasmacytoid dendritic cells, which are the most important type of I IFN producing cells [143, 144]. When the innate immune response is not effective and a delayed-type I IFN response is mounted, the virus cannot be controlled in the early phase of infection and patients are more likely to develop a severe infection. Second, in SARS and MERS infection, the influx of hyperinflammatory cytokines and chemokines is the main cause of lethal outcomes [144, 145]. Huang et al. reported that in COVID-19, higher levels of inflammatory factors were more commonly seen in patients with severe COVID-19 than in those with non-severe COVID-19, suggesting that a cytokine storm was associated with disease severity [8]. Patients with various chronic diseases are already in a proinflammatory state with impaired immune function; hence, the infection can accelerate the inflammatory progress [146]. Therefore, patients with a history of organ dysfunction may have a greater risk of developing severe COVID-19. ...
... ]. When the innate immune response is not effective and a delayed-type I IFN response is mounted, the virus cannot be controlled in the early phase of infection and patients are more likely to develop a severe infection. Second, in SARS and MERS infection, the influx of hyperinflammatory cytokines and chemokines is the main cause of lethal outcomes [144, 145]. Huang et al. reported that in COVID-19, higher levels of inflammatory factors were more commonly seen in patients with severe COVID-19 than in those with non-severe COVID-19, suggesting that a cytokine storm was associated with disease severity [8]. Patients with various chronic diseases are already in a proinflammatory state with impaired immune function; hence, the infection can accelerate the inflammatory progress [146]. Therefore, patients with a history of organ dysfunction may have a greater risk of developing severe COVID-19. ...
... SARS-CoV, MERS-CoV, and SARS-CoV-2 belong to the same genus and all are beta-CoVs. The comparison of genomic sequences revealed that the SARS-CoV-2 genome is 79% and 50% similar to SARS-CoV and MERS-CoV, respectively. SARS-CoV-2 contains additional gene regions, and the amino acid sequences of some SARS-CoV-2 proteins are only 68% similar to those of SARS-CoV [144, 163, 164]. It is reasonable to speculate that SARS-CoV-2 has similar clinical features and pathology as SARS-CoV and MERS-CoV; however, additional characteristics may yet be discovered. These findings reveal that all three coronaviruses might originate in bats prior to mutations. Subsequently they adapt to intermediate hosts and finally to humans [163, 165]. SARS-CoV and SARS-CoV-2 share the cell entry receptor of ACE2, while Dipeptidyl peptidase (DPP)-4 serves as the specific receptor for MERS-CoV [144, 166]. Similar to SARS and MERS, lower respiratory symptoms, including fever, cough, and fatigue, were commonly observed in patients with early-stage COVID-19, while the incidence of GI symptoms was relatively low [17, 141]. In the present study, a history of organ dysfunction was identified as the predictor of severe disease in all three coronaviruses. In addition, the pathological changes in the multiorgan tissues of COVID-19 patients significantly resemble those observed in SARS and MERS infection. This provides evidence for our work [167, 168]. Coronaviruses not only induce direct organ damage but also aggravate the injury through proinflammatory methods. On the basis of the information from previous studies, we found that SARS-CoV-2 shared similarities with SARS-CoV and/or MERS-CoV in various aspects, including genomic sequence, origin, entry receptor, clinical features, risk factors, and pathological processes. As no vaccine or specific treatment with confirmed results is available for treating COVID-19, and COVID-19 has a huge impact, clinical experience from SARS and MERS may provide some guidance regarding treatment strategies that may benefit COVID-19 patients. ...
... ]. SARS-CoV and SARS-CoV-2 share the cell entry receptor of ACE2, while Dipeptidyl peptidase (DPP)-4 serves as the specific receptor for MERS-CoV [144, 166]. Similar to SARS and MERS, lower respiratory symptoms, including fever, cough, and fatigue, were commonly observed in patients with early-stage COVID-19, while the incidence of GI symptoms was relatively low [17, 141]. In the present study, a history of organ dysfunction was identified as the predictor of severe disease in all three coronaviruses. In addition, the pathological changes in the multiorgan tissues of COVID-19 patients significantly resemble those observed in SARS and MERS infection. This provides evidence for our work [167, 168]. Coronaviruses not only induce direct organ damage but also aggravate the injury through proinflammatory methods. On the basis of the information from previous studies, we found that SARS-CoV-2 shared similarities with SARS-CoV and/or MERS-CoV in various aspects, including genomic sequence, origin, entry receptor, clinical features, risk factors, and pathological processes. As no vaccine or specific treatment with confirmed results is available for treating COVID-19, and COVID-19 has a huge impact, clinical experience from SARS and MERS may provide some guidance regarding treatment strategies that may benefit COVID-19 patients. ...
Pathogenic human coronavirus infections: causes and consequences of cytokine storm and immunopathology
1
2017
... However, we assuredly do know that patients with comorbidities such as hypertension, CVD, CKD and COPD, are vulnerable to developing severe disease, which is consistent with previous studies [7, 141]. It can be speculated that comorbidities influence COVID-19 through two mechanisms. First, comorbidities are more prevalent among individuals of advanced age. Innate immunity serves as the first line of defense against pathogen invasion, and successful mounting of type I interferon (IFN) response should be able to suppress viral replication at an early stage [142]. Aging has been reported to impair the capacity of plasmacytoid dendritic cells, which are the most important type of I IFN producing cells [143, 144]. When the innate immune response is not effective and a delayed-type I IFN response is mounted, the virus cannot be controlled in the early phase of infection and patients are more likely to develop a severe infection. Second, in SARS and MERS infection, the influx of hyperinflammatory cytokines and chemokines is the main cause of lethal outcomes [144, 145]. Huang et al. reported that in COVID-19, higher levels of inflammatory factors were more commonly seen in patients with severe COVID-19 than in those with non-severe COVID-19, suggesting that a cytokine storm was associated with disease severity [8]. Patients with various chronic diseases are already in a proinflammatory state with impaired immune function; hence, the infection can accelerate the inflammatory progress [146]. Therefore, patients with a history of organ dysfunction may have a greater risk of developing severe COVID-19. ...
Chronic inflammation in the etiology of disease across the life span
1
2019
... However, we assuredly do know that patients with comorbidities such as hypertension, CVD, CKD and COPD, are vulnerable to developing severe disease, which is consistent with previous studies [7, 141]. It can be speculated that comorbidities influence COVID-19 through two mechanisms. First, comorbidities are more prevalent among individuals of advanced age. Innate immunity serves as the first line of defense against pathogen invasion, and successful mounting of type I interferon (IFN) response should be able to suppress viral replication at an early stage [142]. Aging has been reported to impair the capacity of plasmacytoid dendritic cells, which are the most important type of I IFN producing cells [143, 144]. When the innate immune response is not effective and a delayed-type I IFN response is mounted, the virus cannot be controlled in the early phase of infection and patients are more likely to develop a severe infection. Second, in SARS and MERS infection, the influx of hyperinflammatory cytokines and chemokines is the main cause of lethal outcomes [144, 145]. Huang et al. reported that in COVID-19, higher levels of inflammatory factors were more commonly seen in patients with severe COVID-19 than in those with non-severe COVID-19, suggesting that a cytokine storm was associated with disease severity [8]. Patients with various chronic diseases are already in a proinflammatory state with impaired immune function; hence, the infection can accelerate the inflammatory progress [146]. Therefore, patients with a history of organ dysfunction may have a greater risk of developing severe COVID-19. ...
Caution on Kidney Dysfunctions of COVID-19 Patients
1
2020
... Another key finding is that COVID-19 appears to target multiple organs and induces acute injury. Li et al. found that the condition of patients without AKI at admission could gradually worsen and AKI may be diagnosed during hospitalization [147]. Guo et al. reported that some patients without underlying CVD had elevated TnT levels [148]. In this study, further analysis indicated that the incidence of acute multiorgan injury was considerably higher in patients with severe COVID-19. Similar to SARS-CoV, SARS-CoV-2 uses angiotensin-converting enzyme 2 (ACE2) as the cell entry receptor [149]. Zhao et al. demonstrated that ACE2 was principally expressed in alveolar epithelial type II cells, suggesting that the lung could be the most vulnerable target organ. However, ACE2 is highly expressed in the heart, kidney, liver, brain, and digestive tract, which provides a means for the involvement of multiple organs in COVID-19 [150-152]. Immunostaining of lung tissues indicated that the Rp3 nucleocapsid protein (NP) of SARS-CoV-2 was prominently expressed on alveolar epithelial cells, and histopathological examination revealed all the features of diffuse alveolar damage [103, 153]. Diao et al. found that various degrees of acute tubular necrosis and viral infection-associated syncytia were observed in renal specimens of COVID-19 patients. Furthermore, the NP antigens of SARS-CoV-2 could be observed in kidney tissues [154]. Clusters of coronavirus particles with distinctive spikes were observed in the tubular epithelium and podocytes [155]. No substantial histological changes were identified in the heart [103, 156], however SARS-CoV-2 viral particles have been identified in cardiac tissue in some COVID-19 cases [157, 158]. Biopsy of liver tissues revealed moderate microvesicular steatosis and mild lobular and portal activity; however, the possibility of drug-induced acute liver injury cannot be ruled out [103]. It has been reported that liver injury observed in COVID-19 patients after admission may be caused by LPV/r treatment [104]. Notably, viral RNA was also detected in the liver tissues of COVID-19 patients [158]. Similar to SARS-CoV, SARS-CoV-2 might invade the central nervous system via the nose close to the olfactory epithelium [159]. This was supported by the presence of olfactory disorders in patients with COVID-19. Detectable viral RNA was identified in the brain tissues of some COVID-19 cases [158], and the presence of specific SARS-CoV-2 RNA in COVID-19 patients’ cerebrospinal fluid has also been confirmed [160]. The SARS-CoV-2 RNA and NP were detected in GI tissues from COVID-19 patients [161]. In addition, the successful isolation of SARS-CoV-2 from stool samples demonstrated the fact that there was GI infection [162]. These results suggested that regional viral replication could directly contribute to acute organ damage. Of note, inflammatory cellular infiltration is commonly observed in multiple organs, including the lung, heart, kidney, and liver. This suggests that viruses not only induce direct organ damage but also aggravate the injury through proinflammatory function or cytokine storms [103, 156, 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection. ...
Cardiovascular Implications of Fatal Outcomes of Patients With Coronavirus Disease 2019 (COVID-19)
2
2020
... Another key finding is that COVID-19 appears to target multiple organs and induces acute injury. Li et al. found that the condition of patients without AKI at admission could gradually worsen and AKI may be diagnosed during hospitalization [147]. Guo et al. reported that some patients without underlying CVD had elevated TnT levels [148]. In this study, further analysis indicated that the incidence of acute multiorgan injury was considerably higher in patients with severe COVID-19. Similar to SARS-CoV, SARS-CoV-2 uses angiotensin-converting enzyme 2 (ACE2) as the cell entry receptor [149]. Zhao et al. demonstrated that ACE2 was principally expressed in alveolar epithelial type II cells, suggesting that the lung could be the most vulnerable target organ. However, ACE2 is highly expressed in the heart, kidney, liver, brain, and digestive tract, which provides a means for the involvement of multiple organs in COVID-19 [150-152]. Immunostaining of lung tissues indicated that the Rp3 nucleocapsid protein (NP) of SARS-CoV-2 was prominently expressed on alveolar epithelial cells, and histopathological examination revealed all the features of diffuse alveolar damage [103, 153]. Diao et al. found that various degrees of acute tubular necrosis and viral infection-associated syncytia were observed in renal specimens of COVID-19 patients. Furthermore, the NP antigens of SARS-CoV-2 could be observed in kidney tissues [154]. Clusters of coronavirus particles with distinctive spikes were observed in the tubular epithelium and podocytes [155]. No substantial histological changes were identified in the heart [103, 156], however SARS-CoV-2 viral particles have been identified in cardiac tissue in some COVID-19 cases [157, 158]. Biopsy of liver tissues revealed moderate microvesicular steatosis and mild lobular and portal activity; however, the possibility of drug-induced acute liver injury cannot be ruled out [103]. It has been reported that liver injury observed in COVID-19 patients after admission may be caused by LPV/r treatment [104]. Notably, viral RNA was also detected in the liver tissues of COVID-19 patients [158]. Similar to SARS-CoV, SARS-CoV-2 might invade the central nervous system via the nose close to the olfactory epithelium [159]. This was supported by the presence of olfactory disorders in patients with COVID-19. Detectable viral RNA was identified in the brain tissues of some COVID-19 cases [158], and the presence of specific SARS-CoV-2 RNA in COVID-19 patients’ cerebrospinal fluid has also been confirmed [160]. The SARS-CoV-2 RNA and NP were detected in GI tissues from COVID-19 patients [161]. In addition, the successful isolation of SARS-CoV-2 from stool samples demonstrated the fact that there was GI infection [162]. These results suggested that regional viral replication could directly contribute to acute organ damage. Of note, inflammatory cellular infiltration is commonly observed in multiple organs, including the lung, heart, kidney, and liver. This suggests that viruses not only induce direct organ damage but also aggravate the injury through proinflammatory function or cytokine storms [103, 156, 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection. ...
... In addition, clinicians should be equally alert to patients without organ dysfunction prior to admission. Guo et al. reported that patients with underlying CVD and normal TnT levels had a considerably more favorable outcome than in patients without CVD and with elevated TnT levels [148]. Therefore, it is reasonable to speculate that acute organ injury may play a greater role in the lethal outcome of COVID-19 than a history of organ dysfunction. These results indicate that clinicians should evaluate and prioritize COVID-19 patients according to the presence of organ dysfunction and the evidence of acute organ injury and initiate aggressive treatment. Multiorgan function biomarkers should be closely monitored for early warning and intervention. ...
A pneumonia outbreak associated with a new coronavirus of probable bat origin
1
2020
... Another key finding is that COVID-19 appears to target multiple organs and induces acute injury. Li et al. found that the condition of patients without AKI at admission could gradually worsen and AKI may be diagnosed during hospitalization [147]. Guo et al. reported that some patients without underlying CVD had elevated TnT levels [148]. In this study, further analysis indicated that the incidence of acute multiorgan injury was considerably higher in patients with severe COVID-19. Similar to SARS-CoV, SARS-CoV-2 uses angiotensin-converting enzyme 2 (ACE2) as the cell entry receptor [149]. Zhao et al. demonstrated that ACE2 was principally expressed in alveolar epithelial type II cells, suggesting that the lung could be the most vulnerable target organ. However, ACE2 is highly expressed in the heart, kidney, liver, brain, and digestive tract, which provides a means for the involvement of multiple organs in COVID-19 [150-152]. Immunostaining of lung tissues indicated that the Rp3 nucleocapsid protein (NP) of SARS-CoV-2 was prominently expressed on alveolar epithelial cells, and histopathological examination revealed all the features of diffuse alveolar damage [103, 153]. Diao et al. found that various degrees of acute tubular necrosis and viral infection-associated syncytia were observed in renal specimens of COVID-19 patients. Furthermore, the NP antigens of SARS-CoV-2 could be observed in kidney tissues [154]. Clusters of coronavirus particles with distinctive spikes were observed in the tubular epithelium and podocytes [155]. No substantial histological changes were identified in the heart [103, 156], however SARS-CoV-2 viral particles have been identified in cardiac tissue in some COVID-19 cases [157, 158]. Biopsy of liver tissues revealed moderate microvesicular steatosis and mild lobular and portal activity; however, the possibility of drug-induced acute liver injury cannot be ruled out [103]. It has been reported that liver injury observed in COVID-19 patients after admission may be caused by LPV/r treatment [104]. Notably, viral RNA was also detected in the liver tissues of COVID-19 patients [158]. Similar to SARS-CoV, SARS-CoV-2 might invade the central nervous system via the nose close to the olfactory epithelium [159]. This was supported by the presence of olfactory disorders in patients with COVID-19. Detectable viral RNA was identified in the brain tissues of some COVID-19 cases [158], and the presence of specific SARS-CoV-2 RNA in COVID-19 patients’ cerebrospinal fluid has also been confirmed [160]. The SARS-CoV-2 RNA and NP were detected in GI tissues from COVID-19 patients [161]. In addition, the successful isolation of SARS-CoV-2 from stool samples demonstrated the fact that there was GI infection [162]. These results suggested that regional viral replication could directly contribute to acute organ damage. Of note, inflammatory cellular infiltration is commonly observed in multiple organs, including the lung, heart, kidney, and liver. This suggests that viruses not only induce direct organ damage but also aggravate the injury through proinflammatory function or cytokine storms [103, 156, 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection. ...
Angiotensin-converting enzyme 2 is an essential regulator of heart function
1
2002
... Another key finding is that COVID-19 appears to target multiple organs and induces acute injury. Li et al. found that the condition of patients without AKI at admission could gradually worsen and AKI may be diagnosed during hospitalization [147]. Guo et al. reported that some patients without underlying CVD had elevated TnT levels [148]. In this study, further analysis indicated that the incidence of acute multiorgan injury was considerably higher in patients with severe COVID-19. Similar to SARS-CoV, SARS-CoV-2 uses angiotensin-converting enzyme 2 (ACE2) as the cell entry receptor [149]. Zhao et al. demonstrated that ACE2 was principally expressed in alveolar epithelial type II cells, suggesting that the lung could be the most vulnerable target organ. However, ACE2 is highly expressed in the heart, kidney, liver, brain, and digestive tract, which provides a means for the involvement of multiple organs in COVID-19 [150-152]. Immunostaining of lung tissues indicated that the Rp3 nucleocapsid protein (NP) of SARS-CoV-2 was prominently expressed on alveolar epithelial cells, and histopathological examination revealed all the features of diffuse alveolar damage [103, 153]. Diao et al. found that various degrees of acute tubular necrosis and viral infection-associated syncytia were observed in renal specimens of COVID-19 patients. Furthermore, the NP antigens of SARS-CoV-2 could be observed in kidney tissues [154]. Clusters of coronavirus particles with distinctive spikes were observed in the tubular epithelium and podocytes [155]. No substantial histological changes were identified in the heart [103, 156], however SARS-CoV-2 viral particles have been identified in cardiac tissue in some COVID-19 cases [157, 158]. Biopsy of liver tissues revealed moderate microvesicular steatosis and mild lobular and portal activity; however, the possibility of drug-induced acute liver injury cannot be ruled out [103]. It has been reported that liver injury observed in COVID-19 patients after admission may be caused by LPV/r treatment [104]. Notably, viral RNA was also detected in the liver tissues of COVID-19 patients [158]. Similar to SARS-CoV, SARS-CoV-2 might invade the central nervous system via the nose close to the olfactory epithelium [159]. This was supported by the presence of olfactory disorders in patients with COVID-19. Detectable viral RNA was identified in the brain tissues of some COVID-19 cases [158], and the presence of specific SARS-CoV-2 RNA in COVID-19 patients’ cerebrospinal fluid has also been confirmed [160]. The SARS-CoV-2 RNA and NP were detected in GI tissues from COVID-19 patients [161]. In addition, the successful isolation of SARS-CoV-2 from stool samples demonstrated the fact that there was GI infection [162]. These results suggested that regional viral replication could directly contribute to acute organ damage. Of note, inflammatory cellular infiltration is commonly observed in multiple organs, including the lung, heart, kidney, and liver. This suggests that viruses not only induce direct organ damage but also aggravate the injury through proinflammatory function or cytokine storms [103, 156, 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection. ...
ACE2 Expression in Kidney and Testis May Cause Kidney and Testis Damage After 2019-nCoV Infection
0
2020
Specific ACE2 expression in small intestinal enterocytes may cause gastrointestinal symptoms and injury after 2019-nCoV infection
1
2020
... Another key finding is that COVID-19 appears to target multiple organs and induces acute injury. Li et al. found that the condition of patients without AKI at admission could gradually worsen and AKI may be diagnosed during hospitalization [147]. Guo et al. reported that some patients without underlying CVD had elevated TnT levels [148]. In this study, further analysis indicated that the incidence of acute multiorgan injury was considerably higher in patients with severe COVID-19. Similar to SARS-CoV, SARS-CoV-2 uses angiotensin-converting enzyme 2 (ACE2) as the cell entry receptor [149]. Zhao et al. demonstrated that ACE2 was principally expressed in alveolar epithelial type II cells, suggesting that the lung could be the most vulnerable target organ. However, ACE2 is highly expressed in the heart, kidney, liver, brain, and digestive tract, which provides a means for the involvement of multiple organs in COVID-19 [150-152]. Immunostaining of lung tissues indicated that the Rp3 nucleocapsid protein (NP) of SARS-CoV-2 was prominently expressed on alveolar epithelial cells, and histopathological examination revealed all the features of diffuse alveolar damage [103, 153]. Diao et al. found that various degrees of acute tubular necrosis and viral infection-associated syncytia were observed in renal specimens of COVID-19 patients. Furthermore, the NP antigens of SARS-CoV-2 could be observed in kidney tissues [154]. Clusters of coronavirus particles with distinctive spikes were observed in the tubular epithelium and podocytes [155]. No substantial histological changes were identified in the heart [103, 156], however SARS-CoV-2 viral particles have been identified in cardiac tissue in some COVID-19 cases [157, 158]. Biopsy of liver tissues revealed moderate microvesicular steatosis and mild lobular and portal activity; however, the possibility of drug-induced acute liver injury cannot be ruled out [103]. It has been reported that liver injury observed in COVID-19 patients after admission may be caused by LPV/r treatment [104]. Notably, viral RNA was also detected in the liver tissues of COVID-19 patients [158]. Similar to SARS-CoV, SARS-CoV-2 might invade the central nervous system via the nose close to the olfactory epithelium [159]. This was supported by the presence of olfactory disorders in patients with COVID-19. Detectable viral RNA was identified in the brain tissues of some COVID-19 cases [158], and the presence of specific SARS-CoV-2 RNA in COVID-19 patients’ cerebrospinal fluid has also been confirmed [160]. The SARS-CoV-2 RNA and NP were detected in GI tissues from COVID-19 patients [161]. In addition, the successful isolation of SARS-CoV-2 from stool samples demonstrated the fact that there was GI infection [162]. These results suggested that regional viral replication could directly contribute to acute organ damage. Of note, inflammatory cellular infiltration is commonly observed in multiple organs, including the lung, heart, kidney, and liver. This suggests that viruses not only induce direct organ damage but also aggravate the injury through proinflammatory function or cytokine storms [103, 156, 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection. ...
Histopathologic Changes and SARS-CoV-2 Immunostaining in the Lung of a Patient With COVID-19
1
2020
... Another key finding is that COVID-19 appears to target multiple organs and induces acute injury. Li et al. found that the condition of patients without AKI at admission could gradually worsen and AKI may be diagnosed during hospitalization [147]. Guo et al. reported that some patients without underlying CVD had elevated TnT levels [148]. In this study, further analysis indicated that the incidence of acute multiorgan injury was considerably higher in patients with severe COVID-19. Similar to SARS-CoV, SARS-CoV-2 uses angiotensin-converting enzyme 2 (ACE2) as the cell entry receptor [149]. Zhao et al. demonstrated that ACE2 was principally expressed in alveolar epithelial type II cells, suggesting that the lung could be the most vulnerable target organ. However, ACE2 is highly expressed in the heart, kidney, liver, brain, and digestive tract, which provides a means for the involvement of multiple organs in COVID-19 [150-152]. Immunostaining of lung tissues indicated that the Rp3 nucleocapsid protein (NP) of SARS-CoV-2 was prominently expressed on alveolar epithelial cells, and histopathological examination revealed all the features of diffuse alveolar damage [103, 153]. Diao et al. found that various degrees of acute tubular necrosis and viral infection-associated syncytia were observed in renal specimens of COVID-19 patients. Furthermore, the NP antigens of SARS-CoV-2 could be observed in kidney tissues [154]. Clusters of coronavirus particles with distinctive spikes were observed in the tubular epithelium and podocytes [155]. No substantial histological changes were identified in the heart [103, 156], however SARS-CoV-2 viral particles have been identified in cardiac tissue in some COVID-19 cases [157, 158]. Biopsy of liver tissues revealed moderate microvesicular steatosis and mild lobular and portal activity; however, the possibility of drug-induced acute liver injury cannot be ruled out [103]. It has been reported that liver injury observed in COVID-19 patients after admission may be caused by LPV/r treatment [104]. Notably, viral RNA was also detected in the liver tissues of COVID-19 patients [158]. Similar to SARS-CoV, SARS-CoV-2 might invade the central nervous system via the nose close to the olfactory epithelium [159]. This was supported by the presence of olfactory disorders in patients with COVID-19. Detectable viral RNA was identified in the brain tissues of some COVID-19 cases [158], and the presence of specific SARS-CoV-2 RNA in COVID-19 patients’ cerebrospinal fluid has also been confirmed [160]. The SARS-CoV-2 RNA and NP were detected in GI tissues from COVID-19 patients [161]. In addition, the successful isolation of SARS-CoV-2 from stool samples demonstrated the fact that there was GI infection [162]. These results suggested that regional viral replication could directly contribute to acute organ damage. Of note, inflammatory cellular infiltration is commonly observed in multiple organs, including the lung, heart, kidney, and liver. This suggests that viruses not only induce direct organ damage but also aggravate the injury through proinflammatory function or cytokine storms [103, 156, 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection. ...
Human Kidney is a Target for Novel Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection
1
2020
... Another key finding is that COVID-19 appears to target multiple organs and induces acute injury. Li et al. found that the condition of patients without AKI at admission could gradually worsen and AKI may be diagnosed during hospitalization [147]. Guo et al. reported that some patients without underlying CVD had elevated TnT levels [148]. In this study, further analysis indicated that the incidence of acute multiorgan injury was considerably higher in patients with severe COVID-19. Similar to SARS-CoV, SARS-CoV-2 uses angiotensin-converting enzyme 2 (ACE2) as the cell entry receptor [149]. Zhao et al. demonstrated that ACE2 was principally expressed in alveolar epithelial type II cells, suggesting that the lung could be the most vulnerable target organ. However, ACE2 is highly expressed in the heart, kidney, liver, brain, and digestive tract, which provides a means for the involvement of multiple organs in COVID-19 [150-152]. Immunostaining of lung tissues indicated that the Rp3 nucleocapsid protein (NP) of SARS-CoV-2 was prominently expressed on alveolar epithelial cells, and histopathological examination revealed all the features of diffuse alveolar damage [103, 153]. Diao et al. found that various degrees of acute tubular necrosis and viral infection-associated syncytia were observed in renal specimens of COVID-19 patients. Furthermore, the NP antigens of SARS-CoV-2 could be observed in kidney tissues [154]. Clusters of coronavirus particles with distinctive spikes were observed in the tubular epithelium and podocytes [155]. No substantial histological changes were identified in the heart [103, 156], however SARS-CoV-2 viral particles have been identified in cardiac tissue in some COVID-19 cases [157, 158]. Biopsy of liver tissues revealed moderate microvesicular steatosis and mild lobular and portal activity; however, the possibility of drug-induced acute liver injury cannot be ruled out [103]. It has been reported that liver injury observed in COVID-19 patients after admission may be caused by LPV/r treatment [104]. Notably, viral RNA was also detected in the liver tissues of COVID-19 patients [158]. Similar to SARS-CoV, SARS-CoV-2 might invade the central nervous system via the nose close to the olfactory epithelium [159]. This was supported by the presence of olfactory disorders in patients with COVID-19. Detectable viral RNA was identified in the brain tissues of some COVID-19 cases [158], and the presence of specific SARS-CoV-2 RNA in COVID-19 patients’ cerebrospinal fluid has also been confirmed [160]. The SARS-CoV-2 RNA and NP were detected in GI tissues from COVID-19 patients [161]. In addition, the successful isolation of SARS-CoV-2 from stool samples demonstrated the fact that there was GI infection [162]. These results suggested that regional viral replication could directly contribute to acute organ damage. Of note, inflammatory cellular infiltration is commonly observed in multiple organs, including the lung, heart, kidney, and liver. This suggests that viruses not only induce direct organ damage but also aggravate the injury through proinflammatory function or cytokine storms [103, 156, 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection. ...
Renal histopathological analysis of 26 postmortem findings of patients with COVID-19 in China
1
2020
... Another key finding is that COVID-19 appears to target multiple organs and induces acute injury. Li et al. found that the condition of patients without AKI at admission could gradually worsen and AKI may be diagnosed during hospitalization [147]. Guo et al. reported that some patients without underlying CVD had elevated TnT levels [148]. In this study, further analysis indicated that the incidence of acute multiorgan injury was considerably higher in patients with severe COVID-19. Similar to SARS-CoV, SARS-CoV-2 uses angiotensin-converting enzyme 2 (ACE2) as the cell entry receptor [149]. Zhao et al. demonstrated that ACE2 was principally expressed in alveolar epithelial type II cells, suggesting that the lung could be the most vulnerable target organ. However, ACE2 is highly expressed in the heart, kidney, liver, brain, and digestive tract, which provides a means for the involvement of multiple organs in COVID-19 [150-152]. Immunostaining of lung tissues indicated that the Rp3 nucleocapsid protein (NP) of SARS-CoV-2 was prominently expressed on alveolar epithelial cells, and histopathological examination revealed all the features of diffuse alveolar damage [103, 153]. Diao et al. found that various degrees of acute tubular necrosis and viral infection-associated syncytia were observed in renal specimens of COVID-19 patients. Furthermore, the NP antigens of SARS-CoV-2 could be observed in kidney tissues [154]. Clusters of coronavirus particles with distinctive spikes were observed in the tubular epithelium and podocytes [155]. No substantial histological changes were identified in the heart [103, 156], however SARS-CoV-2 viral particles have been identified in cardiac tissue in some COVID-19 cases [157, 158]. Biopsy of liver tissues revealed moderate microvesicular steatosis and mild lobular and portal activity; however, the possibility of drug-induced acute liver injury cannot be ruled out [103]. It has been reported that liver injury observed in COVID-19 patients after admission may be caused by LPV/r treatment [104]. Notably, viral RNA was also detected in the liver tissues of COVID-19 patients [158]. Similar to SARS-CoV, SARS-CoV-2 might invade the central nervous system via the nose close to the olfactory epithelium [159]. This was supported by the presence of olfactory disorders in patients with COVID-19. Detectable viral RNA was identified in the brain tissues of some COVID-19 cases [158], and the presence of specific SARS-CoV-2 RNA in COVID-19 patients’ cerebrospinal fluid has also been confirmed [160]. The SARS-CoV-2 RNA and NP were detected in GI tissues from COVID-19 patients [161]. In addition, the successful isolation of SARS-CoV-2 from stool samples demonstrated the fact that there was GI infection [162]. These results suggested that regional viral replication could directly contribute to acute organ damage. Of note, inflammatory cellular infiltration is commonly observed in multiple organs, including the lung, heart, kidney, and liver. This suggests that viruses not only induce direct organ damage but also aggravate the injury through proinflammatory function or cytokine storms [103, 156, 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection. ...
Pathological findings of COVID-19 associated with acute respiratory distress syndrome
2
2020
... Another key finding is that COVID-19 appears to target multiple organs and induces acute injury. Li et al. found that the condition of patients without AKI at admission could gradually worsen and AKI may be diagnosed during hospitalization [147]. Guo et al. reported that some patients without underlying CVD had elevated TnT levels [148]. In this study, further analysis indicated that the incidence of acute multiorgan injury was considerably higher in patients with severe COVID-19. Similar to SARS-CoV, SARS-CoV-2 uses angiotensin-converting enzyme 2 (ACE2) as the cell entry receptor [149]. Zhao et al. demonstrated that ACE2 was principally expressed in alveolar epithelial type II cells, suggesting that the lung could be the most vulnerable target organ. However, ACE2 is highly expressed in the heart, kidney, liver, brain, and digestive tract, which provides a means for the involvement of multiple organs in COVID-19 [150-152]. Immunostaining of lung tissues indicated that the Rp3 nucleocapsid protein (NP) of SARS-CoV-2 was prominently expressed on alveolar epithelial cells, and histopathological examination revealed all the features of diffuse alveolar damage [103, 153]. Diao et al. found that various degrees of acute tubular necrosis and viral infection-associated syncytia were observed in renal specimens of COVID-19 patients. Furthermore, the NP antigens of SARS-CoV-2 could be observed in kidney tissues [154]. Clusters of coronavirus particles with distinctive spikes were observed in the tubular epithelium and podocytes [155]. No substantial histological changes were identified in the heart [103, 156], however SARS-CoV-2 viral particles have been identified in cardiac tissue in some COVID-19 cases [157, 158]. Biopsy of liver tissues revealed moderate microvesicular steatosis and mild lobular and portal activity; however, the possibility of drug-induced acute liver injury cannot be ruled out [103]. It has been reported that liver injury observed in COVID-19 patients after admission may be caused by LPV/r treatment [104]. Notably, viral RNA was also detected in the liver tissues of COVID-19 patients [158]. Similar to SARS-CoV, SARS-CoV-2 might invade the central nervous system via the nose close to the olfactory epithelium [159]. This was supported by the presence of olfactory disorders in patients with COVID-19. Detectable viral RNA was identified in the brain tissues of some COVID-19 cases [158], and the presence of specific SARS-CoV-2 RNA in COVID-19 patients’ cerebrospinal fluid has also been confirmed [160]. The SARS-CoV-2 RNA and NP were detected in GI tissues from COVID-19 patients [161]. In addition, the successful isolation of SARS-CoV-2 from stool samples demonstrated the fact that there was GI infection [162]. These results suggested that regional viral replication could directly contribute to acute organ damage. Of note, inflammatory cellular infiltration is commonly observed in multiple organs, including the lung, heart, kidney, and liver. This suggests that viruses not only induce direct organ damage but also aggravate the injury through proinflammatory function or cytokine storms [103, 156, 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection. ...
... , 156, 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection. ...
A pathological report of three COVID-19 cases by minimally invasive autopsies
1
2020
... Another key finding is that COVID-19 appears to target multiple organs and induces acute injury. Li et al. found that the condition of patients without AKI at admission could gradually worsen and AKI may be diagnosed during hospitalization [147]. Guo et al. reported that some patients without underlying CVD had elevated TnT levels [148]. In this study, further analysis indicated that the incidence of acute multiorgan injury was considerably higher in patients with severe COVID-19. Similar to SARS-CoV, SARS-CoV-2 uses angiotensin-converting enzyme 2 (ACE2) as the cell entry receptor [149]. Zhao et al. demonstrated that ACE2 was principally expressed in alveolar epithelial type II cells, suggesting that the lung could be the most vulnerable target organ. However, ACE2 is highly expressed in the heart, kidney, liver, brain, and digestive tract, which provides a means for the involvement of multiple organs in COVID-19 [150-152]. Immunostaining of lung tissues indicated that the Rp3 nucleocapsid protein (NP) of SARS-CoV-2 was prominently expressed on alveolar epithelial cells, and histopathological examination revealed all the features of diffuse alveolar damage [103, 153]. Diao et al. found that various degrees of acute tubular necrosis and viral infection-associated syncytia were observed in renal specimens of COVID-19 patients. Furthermore, the NP antigens of SARS-CoV-2 could be observed in kidney tissues [154]. Clusters of coronavirus particles with distinctive spikes were observed in the tubular epithelium and podocytes [155]. No substantial histological changes were identified in the heart [103, 156], however SARS-CoV-2 viral particles have been identified in cardiac tissue in some COVID-19 cases [157, 158]. Biopsy of liver tissues revealed moderate microvesicular steatosis and mild lobular and portal activity; however, the possibility of drug-induced acute liver injury cannot be ruled out [103]. It has been reported that liver injury observed in COVID-19 patients after admission may be caused by LPV/r treatment [104]. Notably, viral RNA was also detected in the liver tissues of COVID-19 patients [158]. Similar to SARS-CoV, SARS-CoV-2 might invade the central nervous system via the nose close to the olfactory epithelium [159]. This was supported by the presence of olfactory disorders in patients with COVID-19. Detectable viral RNA was identified in the brain tissues of some COVID-19 cases [158], and the presence of specific SARS-CoV-2 RNA in COVID-19 patients’ cerebrospinal fluid has also been confirmed [160]. The SARS-CoV-2 RNA and NP were detected in GI tissues from COVID-19 patients [161]. In addition, the successful isolation of SARS-CoV-2 from stool samples demonstrated the fact that there was GI infection [162]. These results suggested that regional viral replication could directly contribute to acute organ damage. Of note, inflammatory cellular infiltration is commonly observed in multiple organs, including the lung, heart, kidney, and liver. This suggests that viruses not only induce direct organ damage but also aggravate the injury through proinflammatory function or cytokine storms [103, 156, 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection. ...
Autopsy Findings and Venous Thromboembolism in Patients With COVID-19: A Prospective Cohort Study
4
2020
... Another key finding is that COVID-19 appears to target multiple organs and induces acute injury. Li et al. found that the condition of patients without AKI at admission could gradually worsen and AKI may be diagnosed during hospitalization [147]. Guo et al. reported that some patients without underlying CVD had elevated TnT levels [148]. In this study, further analysis indicated that the incidence of acute multiorgan injury was considerably higher in patients with severe COVID-19. Similar to SARS-CoV, SARS-CoV-2 uses angiotensin-converting enzyme 2 (ACE2) as the cell entry receptor [149]. Zhao et al. demonstrated that ACE2 was principally expressed in alveolar epithelial type II cells, suggesting that the lung could be the most vulnerable target organ. However, ACE2 is highly expressed in the heart, kidney, liver, brain, and digestive tract, which provides a means for the involvement of multiple organs in COVID-19 [150-152]. Immunostaining of lung tissues indicated that the Rp3 nucleocapsid protein (NP) of SARS-CoV-2 was prominently expressed on alveolar epithelial cells, and histopathological examination revealed all the features of diffuse alveolar damage [103, 153]. Diao et al. found that various degrees of acute tubular necrosis and viral infection-associated syncytia were observed in renal specimens of COVID-19 patients. Furthermore, the NP antigens of SARS-CoV-2 could be observed in kidney tissues [154]. Clusters of coronavirus particles with distinctive spikes were observed in the tubular epithelium and podocytes [155]. No substantial histological changes were identified in the heart [103, 156], however SARS-CoV-2 viral particles have been identified in cardiac tissue in some COVID-19 cases [157, 158]. Biopsy of liver tissues revealed moderate microvesicular steatosis and mild lobular and portal activity; however, the possibility of drug-induced acute liver injury cannot be ruled out [103]. It has been reported that liver injury observed in COVID-19 patients after admission may be caused by LPV/r treatment [104]. Notably, viral RNA was also detected in the liver tissues of COVID-19 patients [158]. Similar to SARS-CoV, SARS-CoV-2 might invade the central nervous system via the nose close to the olfactory epithelium [159]. This was supported by the presence of olfactory disorders in patients with COVID-19. Detectable viral RNA was identified in the brain tissues of some COVID-19 cases [158], and the presence of specific SARS-CoV-2 RNA in COVID-19 patients’ cerebrospinal fluid has also been confirmed [160]. The SARS-CoV-2 RNA and NP were detected in GI tissues from COVID-19 patients [161]. In addition, the successful isolation of SARS-CoV-2 from stool samples demonstrated the fact that there was GI infection [162]. These results suggested that regional viral replication could directly contribute to acute organ damage. Of note, inflammatory cellular infiltration is commonly observed in multiple organs, including the lung, heart, kidney, and liver. This suggests that viruses not only induce direct organ damage but also aggravate the injury through proinflammatory function or cytokine storms [103, 156, 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection. ...
... ]. Notably, viral RNA was also detected in the liver tissues of COVID-19 patients [158]. Similar to SARS-CoV, SARS-CoV-2 might invade the central nervous system via the nose close to the olfactory epithelium [159]. This was supported by the presence of olfactory disorders in patients with COVID-19. Detectable viral RNA was identified in the brain tissues of some COVID-19 cases [158], and the presence of specific SARS-CoV-2 RNA in COVID-19 patients’ cerebrospinal fluid has also been confirmed [160]. The SARS-CoV-2 RNA and NP were detected in GI tissues from COVID-19 patients [161]. In addition, the successful isolation of SARS-CoV-2 from stool samples demonstrated the fact that there was GI infection [162]. These results suggested that regional viral replication could directly contribute to acute organ damage. Of note, inflammatory cellular infiltration is commonly observed in multiple organs, including the lung, heart, kidney, and liver. This suggests that viruses not only induce direct organ damage but also aggravate the injury through proinflammatory function or cytokine storms [103, 156, 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection. ...
... ]. This was supported by the presence of olfactory disorders in patients with COVID-19. Detectable viral RNA was identified in the brain tissues of some COVID-19 cases [158], and the presence of specific SARS-CoV-2 RNA in COVID-19 patients’ cerebrospinal fluid has also been confirmed [160]. The SARS-CoV-2 RNA and NP were detected in GI tissues from COVID-19 patients [161]. In addition, the successful isolation of SARS-CoV-2 from stool samples demonstrated the fact that there was GI infection [162]. These results suggested that regional viral replication could directly contribute to acute organ damage. Of note, inflammatory cellular infiltration is commonly observed in multiple organs, including the lung, heart, kidney, and liver. This suggests that viruses not only induce direct organ damage but also aggravate the injury through proinflammatory function or cytokine storms [103, 156, 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection. ...
... , 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection. ...
Severe acute respiratory syndrome coronavirus infection causes neuronal death in the absence of encephalitis in mice transgenic for human ACE2
1
2008
... Another key finding is that COVID-19 appears to target multiple organs and induces acute injury. Li et al. found that the condition of patients without AKI at admission could gradually worsen and AKI may be diagnosed during hospitalization [147]. Guo et al. reported that some patients without underlying CVD had elevated TnT levels [148]. In this study, further analysis indicated that the incidence of acute multiorgan injury was considerably higher in patients with severe COVID-19. Similar to SARS-CoV, SARS-CoV-2 uses angiotensin-converting enzyme 2 (ACE2) as the cell entry receptor [149]. Zhao et al. demonstrated that ACE2 was principally expressed in alveolar epithelial type II cells, suggesting that the lung could be the most vulnerable target organ. However, ACE2 is highly expressed in the heart, kidney, liver, brain, and digestive tract, which provides a means for the involvement of multiple organs in COVID-19 [150-152]. Immunostaining of lung tissues indicated that the Rp3 nucleocapsid protein (NP) of SARS-CoV-2 was prominently expressed on alveolar epithelial cells, and histopathological examination revealed all the features of diffuse alveolar damage [103, 153]. Diao et al. found that various degrees of acute tubular necrosis and viral infection-associated syncytia were observed in renal specimens of COVID-19 patients. Furthermore, the NP antigens of SARS-CoV-2 could be observed in kidney tissues [154]. Clusters of coronavirus particles with distinctive spikes were observed in the tubular epithelium and podocytes [155]. No substantial histological changes were identified in the heart [103, 156], however SARS-CoV-2 viral particles have been identified in cardiac tissue in some COVID-19 cases [157, 158]. Biopsy of liver tissues revealed moderate microvesicular steatosis and mild lobular and portal activity; however, the possibility of drug-induced acute liver injury cannot be ruled out [103]. It has been reported that liver injury observed in COVID-19 patients after admission may be caused by LPV/r treatment [104]. Notably, viral RNA was also detected in the liver tissues of COVID-19 patients [158]. Similar to SARS-CoV, SARS-CoV-2 might invade the central nervous system via the nose close to the olfactory epithelium [159]. This was supported by the presence of olfactory disorders in patients with COVID-19. Detectable viral RNA was identified in the brain tissues of some COVID-19 cases [158], and the presence of specific SARS-CoV-2 RNA in COVID-19 patients’ cerebrospinal fluid has also been confirmed [160]. The SARS-CoV-2 RNA and NP were detected in GI tissues from COVID-19 patients [161]. In addition, the successful isolation of SARS-CoV-2 from stool samples demonstrated the fact that there was GI infection [162]. These results suggested that regional viral replication could directly contribute to acute organ damage. Of note, inflammatory cellular infiltration is commonly observed in multiple organs, including the lung, heart, kidney, and liver. This suggests that viruses not only induce direct organ damage but also aggravate the injury through proinflammatory function or cytokine storms [103, 156, 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection. ...
A first case of meningitis/encephalitis associated with SARS-Coronavirus-2
1
2020
... Another key finding is that COVID-19 appears to target multiple organs and induces acute injury. Li et al. found that the condition of patients without AKI at admission could gradually worsen and AKI may be diagnosed during hospitalization [147]. Guo et al. reported that some patients without underlying CVD had elevated TnT levels [148]. In this study, further analysis indicated that the incidence of acute multiorgan injury was considerably higher in patients with severe COVID-19. Similar to SARS-CoV, SARS-CoV-2 uses angiotensin-converting enzyme 2 (ACE2) as the cell entry receptor [149]. Zhao et al. demonstrated that ACE2 was principally expressed in alveolar epithelial type II cells, suggesting that the lung could be the most vulnerable target organ. However, ACE2 is highly expressed in the heart, kidney, liver, brain, and digestive tract, which provides a means for the involvement of multiple organs in COVID-19 [150-152]. Immunostaining of lung tissues indicated that the Rp3 nucleocapsid protein (NP) of SARS-CoV-2 was prominently expressed on alveolar epithelial cells, and histopathological examination revealed all the features of diffuse alveolar damage [103, 153]. Diao et al. found that various degrees of acute tubular necrosis and viral infection-associated syncytia were observed in renal specimens of COVID-19 patients. Furthermore, the NP antigens of SARS-CoV-2 could be observed in kidney tissues [154]. Clusters of coronavirus particles with distinctive spikes were observed in the tubular epithelium and podocytes [155]. No substantial histological changes were identified in the heart [103, 156], however SARS-CoV-2 viral particles have been identified in cardiac tissue in some COVID-19 cases [157, 158]. Biopsy of liver tissues revealed moderate microvesicular steatosis and mild lobular and portal activity; however, the possibility of drug-induced acute liver injury cannot be ruled out [103]. It has been reported that liver injury observed in COVID-19 patients after admission may be caused by LPV/r treatment [104]. Notably, viral RNA was also detected in the liver tissues of COVID-19 patients [158]. Similar to SARS-CoV, SARS-CoV-2 might invade the central nervous system via the nose close to the olfactory epithelium [159]. This was supported by the presence of olfactory disorders in patients with COVID-19. Detectable viral RNA was identified in the brain tissues of some COVID-19 cases [158], and the presence of specific SARS-CoV-2 RNA in COVID-19 patients’ cerebrospinal fluid has also been confirmed [160]. The SARS-CoV-2 RNA and NP were detected in GI tissues from COVID-19 patients [161]. In addition, the successful isolation of SARS-CoV-2 from stool samples demonstrated the fact that there was GI infection [162]. These results suggested that regional viral replication could directly contribute to acute organ damage. Of note, inflammatory cellular infiltration is commonly observed in multiple organs, including the lung, heart, kidney, and liver. This suggests that viruses not only induce direct organ damage but also aggravate the injury through proinflammatory function or cytokine storms [103, 156, 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection. ...
Evidence for Gastrointestinal Infection of SARS-CoV-2
1
2020
... Another key finding is that COVID-19 appears to target multiple organs and induces acute injury. Li et al. found that the condition of patients without AKI at admission could gradually worsen and AKI may be diagnosed during hospitalization [147]. Guo et al. reported that some patients without underlying CVD had elevated TnT levels [148]. In this study, further analysis indicated that the incidence of acute multiorgan injury was considerably higher in patients with severe COVID-19. Similar to SARS-CoV, SARS-CoV-2 uses angiotensin-converting enzyme 2 (ACE2) as the cell entry receptor [149]. Zhao et al. demonstrated that ACE2 was principally expressed in alveolar epithelial type II cells, suggesting that the lung could be the most vulnerable target organ. However, ACE2 is highly expressed in the heart, kidney, liver, brain, and digestive tract, which provides a means for the involvement of multiple organs in COVID-19 [150-152]. Immunostaining of lung tissues indicated that the Rp3 nucleocapsid protein (NP) of SARS-CoV-2 was prominently expressed on alveolar epithelial cells, and histopathological examination revealed all the features of diffuse alveolar damage [103, 153]. Diao et al. found that various degrees of acute tubular necrosis and viral infection-associated syncytia were observed in renal specimens of COVID-19 patients. Furthermore, the NP antigens of SARS-CoV-2 could be observed in kidney tissues [154]. Clusters of coronavirus particles with distinctive spikes were observed in the tubular epithelium and podocytes [155]. No substantial histological changes were identified in the heart [103, 156], however SARS-CoV-2 viral particles have been identified in cardiac tissue in some COVID-19 cases [157, 158]. Biopsy of liver tissues revealed moderate microvesicular steatosis and mild lobular and portal activity; however, the possibility of drug-induced acute liver injury cannot be ruled out [103]. It has been reported that liver injury observed in COVID-19 patients after admission may be caused by LPV/r treatment [104]. Notably, viral RNA was also detected in the liver tissues of COVID-19 patients [158]. Similar to SARS-CoV, SARS-CoV-2 might invade the central nervous system via the nose close to the olfactory epithelium [159]. This was supported by the presence of olfactory disorders in patients with COVID-19. Detectable viral RNA was identified in the brain tissues of some COVID-19 cases [158], and the presence of specific SARS-CoV-2 RNA in COVID-19 patients’ cerebrospinal fluid has also been confirmed [160]. The SARS-CoV-2 RNA and NP were detected in GI tissues from COVID-19 patients [161]. In addition, the successful isolation of SARS-CoV-2 from stool samples demonstrated the fact that there was GI infection [162]. These results suggested that regional viral replication could directly contribute to acute organ damage. Of note, inflammatory cellular infiltration is commonly observed in multiple organs, including the lung, heart, kidney, and liver. This suggests that viruses not only induce direct organ damage but also aggravate the injury through proinflammatory function or cytokine storms [103, 156, 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection. ...
Isolation of 2019-nCoV from a Stool Specimen of a Laboratory-Confirmed Case of the Coronavirus Disease 2019 (COVID-19)
1
2020
... Another key finding is that COVID-19 appears to target multiple organs and induces acute injury. Li et al. found that the condition of patients without AKI at admission could gradually worsen and AKI may be diagnosed during hospitalization [147]. Guo et al. reported that some patients without underlying CVD had elevated TnT levels [148]. In this study, further analysis indicated that the incidence of acute multiorgan injury was considerably higher in patients with severe COVID-19. Similar to SARS-CoV, SARS-CoV-2 uses angiotensin-converting enzyme 2 (ACE2) as the cell entry receptor [149]. Zhao et al. demonstrated that ACE2 was principally expressed in alveolar epithelial type II cells, suggesting that the lung could be the most vulnerable target organ. However, ACE2 is highly expressed in the heart, kidney, liver, brain, and digestive tract, which provides a means for the involvement of multiple organs in COVID-19 [150-152]. Immunostaining of lung tissues indicated that the Rp3 nucleocapsid protein (NP) of SARS-CoV-2 was prominently expressed on alveolar epithelial cells, and histopathological examination revealed all the features of diffuse alveolar damage [103, 153]. Diao et al. found that various degrees of acute tubular necrosis and viral infection-associated syncytia were observed in renal specimens of COVID-19 patients. Furthermore, the NP antigens of SARS-CoV-2 could be observed in kidney tissues [154]. Clusters of coronavirus particles with distinctive spikes were observed in the tubular epithelium and podocytes [155]. No substantial histological changes were identified in the heart [103, 156], however SARS-CoV-2 viral particles have been identified in cardiac tissue in some COVID-19 cases [157, 158]. Biopsy of liver tissues revealed moderate microvesicular steatosis and mild lobular and portal activity; however, the possibility of drug-induced acute liver injury cannot be ruled out [103]. It has been reported that liver injury observed in COVID-19 patients after admission may be caused by LPV/r treatment [104]. Notably, viral RNA was also detected in the liver tissues of COVID-19 patients [158]. Similar to SARS-CoV, SARS-CoV-2 might invade the central nervous system via the nose close to the olfactory epithelium [159]. This was supported by the presence of olfactory disorders in patients with COVID-19. Detectable viral RNA was identified in the brain tissues of some COVID-19 cases [158], and the presence of specific SARS-CoV-2 RNA in COVID-19 patients’ cerebrospinal fluid has also been confirmed [160]. The SARS-CoV-2 RNA and NP were detected in GI tissues from COVID-19 patients [161]. In addition, the successful isolation of SARS-CoV-2 from stool samples demonstrated the fact that there was GI infection [162]. These results suggested that regional viral replication could directly contribute to acute organ damage. Of note, inflammatory cellular infiltration is commonly observed in multiple organs, including the lung, heart, kidney, and liver. This suggests that viruses not only induce direct organ damage but also aggravate the injury through proinflammatory function or cytokine storms [103, 156, 158]. Furthermore, the prevalence of a history of multiple organ dysfunction was also likely to partially explain the more frequent incidence of acute organ damage in severe COVID-19 patients. Besides, the effects of systemic hypoxia and abnormal coagulation could not be ruled out. According to our study results and the evidence from other studies, we strongly suggest that clinicians should be alert to the monitoring and protecting of extrapulmonary multiple organ function in COVID-19 patients in the early stage of infection. ...
Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding
2
2020
... SARS-CoV, MERS-CoV, and SARS-CoV-2 belong to the same genus and all are beta-CoVs. The comparison of genomic sequences revealed that the SARS-CoV-2 genome is 79% and 50% similar to SARS-CoV and MERS-CoV, respectively. SARS-CoV-2 contains additional gene regions, and the amino acid sequences of some SARS-CoV-2 proteins are only 68% similar to those of SARS-CoV [144, 163, 164]. It is reasonable to speculate that SARS-CoV-2 has similar clinical features and pathology as SARS-CoV and MERS-CoV; however, additional characteristics may yet be discovered. These findings reveal that all three coronaviruses might originate in bats prior to mutations. Subsequently they adapt to intermediate hosts and finally to humans [163, 165]. SARS-CoV and SARS-CoV-2 share the cell entry receptor of ACE2, while Dipeptidyl peptidase (DPP)-4 serves as the specific receptor for MERS-CoV [144, 166]. Similar to SARS and MERS, lower respiratory symptoms, including fever, cough, and fatigue, were commonly observed in patients with early-stage COVID-19, while the incidence of GI symptoms was relatively low [17, 141]. In the present study, a history of organ dysfunction was identified as the predictor of severe disease in all three coronaviruses. In addition, the pathological changes in the multiorgan tissues of COVID-19 patients significantly resemble those observed in SARS and MERS infection. This provides evidence for our work [167, 168]. Coronaviruses not only induce direct organ damage but also aggravate the injury through proinflammatory methods. On the basis of the information from previous studies, we found that SARS-CoV-2 shared similarities with SARS-CoV and/or MERS-CoV in various aspects, including genomic sequence, origin, entry receptor, clinical features, risk factors, and pathological processes. As no vaccine or specific treatment with confirmed results is available for treating COVID-19, and COVID-19 has a huge impact, clinical experience from SARS and MERS may provide some guidance regarding treatment strategies that may benefit COVID-19 patients. ...
... ]. It is reasonable to speculate that SARS-CoV-2 has similar clinical features and pathology as SARS-CoV and MERS-CoV; however, additional characteristics may yet be discovered. These findings reveal that all three coronaviruses might originate in bats prior to mutations. Subsequently they adapt to intermediate hosts and finally to humans [163, 165]. SARS-CoV and SARS-CoV-2 share the cell entry receptor of ACE2, while Dipeptidyl peptidase (DPP)-4 serves as the specific receptor for MERS-CoV [144, 166]. Similar to SARS and MERS, lower respiratory symptoms, including fever, cough, and fatigue, were commonly observed in patients with early-stage COVID-19, while the incidence of GI symptoms was relatively low [17, 141]. In the present study, a history of organ dysfunction was identified as the predictor of severe disease in all three coronaviruses. In addition, the pathological changes in the multiorgan tissues of COVID-19 patients significantly resemble those observed in SARS and MERS infection. This provides evidence for our work [167, 168]. Coronaviruses not only induce direct organ damage but also aggravate the injury through proinflammatory methods. On the basis of the information from previous studies, we found that SARS-CoV-2 shared similarities with SARS-CoV and/or MERS-CoV in various aspects, including genomic sequence, origin, entry receptor, clinical features, risk factors, and pathological processes. As no vaccine or specific treatment with confirmed results is available for treating COVID-19, and COVID-19 has a huge impact, clinical experience from SARS and MERS may provide some guidance regarding treatment strategies that may benefit COVID-19 patients. ...
Recent progress in understanding 2019 novel coronavirus (SARS-CoV-2) associated with human respiratory disease: detection, mechanisms and treatment
1
2020
... SARS-CoV, MERS-CoV, and SARS-CoV-2 belong to the same genus and all are beta-CoVs. The comparison of genomic sequences revealed that the SARS-CoV-2 genome is 79% and 50% similar to SARS-CoV and MERS-CoV, respectively. SARS-CoV-2 contains additional gene regions, and the amino acid sequences of some SARS-CoV-2 proteins are only 68% similar to those of SARS-CoV [144, 163, 164]. It is reasonable to speculate that SARS-CoV-2 has similar clinical features and pathology as SARS-CoV and MERS-CoV; however, additional characteristics may yet be discovered. These findings reveal that all three coronaviruses might originate in bats prior to mutations. Subsequently they adapt to intermediate hosts and finally to humans [163, 165]. SARS-CoV and SARS-CoV-2 share the cell entry receptor of ACE2, while Dipeptidyl peptidase (DPP)-4 serves as the specific receptor for MERS-CoV [144, 166]. Similar to SARS and MERS, lower respiratory symptoms, including fever, cough, and fatigue, were commonly observed in patients with early-stage COVID-19, while the incidence of GI symptoms was relatively low [17, 141]. In the present study, a history of organ dysfunction was identified as the predictor of severe disease in all three coronaviruses. In addition, the pathological changes in the multiorgan tissues of COVID-19 patients significantly resemble those observed in SARS and MERS infection. This provides evidence for our work [167, 168]. Coronaviruses not only induce direct organ damage but also aggravate the injury through proinflammatory methods. On the basis of the information from previous studies, we found that SARS-CoV-2 shared similarities with SARS-CoV and/or MERS-CoV in various aspects, including genomic sequence, origin, entry receptor, clinical features, risk factors, and pathological processes. As no vaccine or specific treatment with confirmed results is available for treating COVID-19, and COVID-19 has a huge impact, clinical experience from SARS and MERS may provide some guidance regarding treatment strategies that may benefit COVID-19 patients. ...
Middle East respiratory syndrome coronavirus infection in dromedary camels in Saudi Arabia
1
2014
... SARS-CoV, MERS-CoV, and SARS-CoV-2 belong to the same genus and all are beta-CoVs. The comparison of genomic sequences revealed that the SARS-CoV-2 genome is 79% and 50% similar to SARS-CoV and MERS-CoV, respectively. SARS-CoV-2 contains additional gene regions, and the amino acid sequences of some SARS-CoV-2 proteins are only 68% similar to those of SARS-CoV [144, 163, 164]. It is reasonable to speculate that SARS-CoV-2 has similar clinical features and pathology as SARS-CoV and MERS-CoV; however, additional characteristics may yet be discovered. These findings reveal that all three coronaviruses might originate in bats prior to mutations. Subsequently they adapt to intermediate hosts and finally to humans [163, 165]. SARS-CoV and SARS-CoV-2 share the cell entry receptor of ACE2, while Dipeptidyl peptidase (DPP)-4 serves as the specific receptor for MERS-CoV [144, 166]. Similar to SARS and MERS, lower respiratory symptoms, including fever, cough, and fatigue, were commonly observed in patients with early-stage COVID-19, while the incidence of GI symptoms was relatively low [17, 141]. In the present study, a history of organ dysfunction was identified as the predictor of severe disease in all three coronaviruses. In addition, the pathological changes in the multiorgan tissues of COVID-19 patients significantly resemble those observed in SARS and MERS infection. This provides evidence for our work [167, 168]. Coronaviruses not only induce direct organ damage but also aggravate the injury through proinflammatory methods. On the basis of the information from previous studies, we found that SARS-CoV-2 shared similarities with SARS-CoV and/or MERS-CoV in various aspects, including genomic sequence, origin, entry receptor, clinical features, risk factors, and pathological processes. As no vaccine or specific treatment with confirmed results is available for treating COVID-19, and COVID-19 has a huge impact, clinical experience from SARS and MERS may provide some guidance regarding treatment strategies that may benefit COVID-19 patients. ...
Structure of MERS-CoV spike receptor-binding domain complexed with human receptor DPP4
1
2013
... SARS-CoV, MERS-CoV, and SARS-CoV-2 belong to the same genus and all are beta-CoVs. The comparison of genomic sequences revealed that the SARS-CoV-2 genome is 79% and 50% similar to SARS-CoV and MERS-CoV, respectively. SARS-CoV-2 contains additional gene regions, and the amino acid sequences of some SARS-CoV-2 proteins are only 68% similar to those of SARS-CoV [144, 163, 164]. It is reasonable to speculate that SARS-CoV-2 has similar clinical features and pathology as SARS-CoV and MERS-CoV; however, additional characteristics may yet be discovered. These findings reveal that all three coronaviruses might originate in bats prior to mutations. Subsequently they adapt to intermediate hosts and finally to humans [163, 165]. SARS-CoV and SARS-CoV-2 share the cell entry receptor of ACE2, while Dipeptidyl peptidase (DPP)-4 serves as the specific receptor for MERS-CoV [144, 166]. Similar to SARS and MERS, lower respiratory symptoms, including fever, cough, and fatigue, were commonly observed in patients with early-stage COVID-19, while the incidence of GI symptoms was relatively low [17, 141]. In the present study, a history of organ dysfunction was identified as the predictor of severe disease in all three coronaviruses. In addition, the pathological changes in the multiorgan tissues of COVID-19 patients significantly resemble those observed in SARS and MERS infection. This provides evidence for our work [167, 168]. Coronaviruses not only induce direct organ damage but also aggravate the injury through proinflammatory methods. On the basis of the information from previous studies, we found that SARS-CoV-2 shared similarities with SARS-CoV and/or MERS-CoV in various aspects, including genomic sequence, origin, entry receptor, clinical features, risk factors, and pathological processes. As no vaccine or specific treatment with confirmed results is available for treating COVID-19, and COVID-19 has a huge impact, clinical experience from SARS and MERS may provide some guidance regarding treatment strategies that may benefit COVID-19 patients. ...
The clinical pathology of severe acute respiratory syndrome (SARS): a report from China
1
2003
... SARS-CoV, MERS-CoV, and SARS-CoV-2 belong to the same genus and all are beta-CoVs. The comparison of genomic sequences revealed that the SARS-CoV-2 genome is 79% and 50% similar to SARS-CoV and MERS-CoV, respectively. SARS-CoV-2 contains additional gene regions, and the amino acid sequences of some SARS-CoV-2 proteins are only 68% similar to those of SARS-CoV [144, 163, 164]. It is reasonable to speculate that SARS-CoV-2 has similar clinical features and pathology as SARS-CoV and MERS-CoV; however, additional characteristics may yet be discovered. These findings reveal that all three coronaviruses might originate in bats prior to mutations. Subsequently they adapt to intermediate hosts and finally to humans [163, 165]. SARS-CoV and SARS-CoV-2 share the cell entry receptor of ACE2, while Dipeptidyl peptidase (DPP)-4 serves as the specific receptor for MERS-CoV [144, 166]. Similar to SARS and MERS, lower respiratory symptoms, including fever, cough, and fatigue, were commonly observed in patients with early-stage COVID-19, while the incidence of GI symptoms was relatively low [17, 141]. In the present study, a history of organ dysfunction was identified as the predictor of severe disease in all three coronaviruses. In addition, the pathological changes in the multiorgan tissues of COVID-19 patients significantly resemble those observed in SARS and MERS infection. This provides evidence for our work [167, 168]. Coronaviruses not only induce direct organ damage but also aggravate the injury through proinflammatory methods. On the basis of the information from previous studies, we found that SARS-CoV-2 shared similarities with SARS-CoV and/or MERS-CoV in various aspects, including genomic sequence, origin, entry receptor, clinical features, risk factors, and pathological processes. As no vaccine or specific treatment with confirmed results is available for treating COVID-19, and COVID-19 has a huge impact, clinical experience from SARS and MERS may provide some guidance regarding treatment strategies that may benefit COVID-19 patients. ...
Clinicopathologic, Immunohistochemical, and Ultrastructural Findings of a Fatal Case of Middle East Respiratory Syndrome Coronavirus Infection in the United Arab Emirates, April 2014
1
2016
... SARS-CoV, MERS-CoV, and SARS-CoV-2 belong to the same genus and all are beta-CoVs. The comparison of genomic sequences revealed that the SARS-CoV-2 genome is 79% and 50% similar to SARS-CoV and MERS-CoV, respectively. SARS-CoV-2 contains additional gene regions, and the amino acid sequences of some SARS-CoV-2 proteins are only 68% similar to those of SARS-CoV [144, 163, 164]. It is reasonable to speculate that SARS-CoV-2 has similar clinical features and pathology as SARS-CoV and MERS-CoV; however, additional characteristics may yet be discovered. These findings reveal that all three coronaviruses might originate in bats prior to mutations. Subsequently they adapt to intermediate hosts and finally to humans [163, 165]. SARS-CoV and SARS-CoV-2 share the cell entry receptor of ACE2, while Dipeptidyl peptidase (DPP)-4 serves as the specific receptor for MERS-CoV [144, 166]. Similar to SARS and MERS, lower respiratory symptoms, including fever, cough, and fatigue, were commonly observed in patients with early-stage COVID-19, while the incidence of GI symptoms was relatively low [17, 141]. In the present study, a history of organ dysfunction was identified as the predictor of severe disease in all three coronaviruses. In addition, the pathological changes in the multiorgan tissues of COVID-19 patients significantly resemble those observed in SARS and MERS infection. This provides evidence for our work [167, 168]. Coronaviruses not only induce direct organ damage but also aggravate the injury through proinflammatory methods. On the basis of the information from previous studies, we found that SARS-CoV-2 shared similarities with SARS-CoV and/or MERS-CoV in various aspects, including genomic sequence, origin, entry receptor, clinical features, risk factors, and pathological processes. As no vaccine or specific treatment with confirmed results is available for treating COVID-19, and COVID-19 has a huge impact, clinical experience from SARS and MERS may provide some guidance regarding treatment strategies that may benefit COVID-19 patients. ...
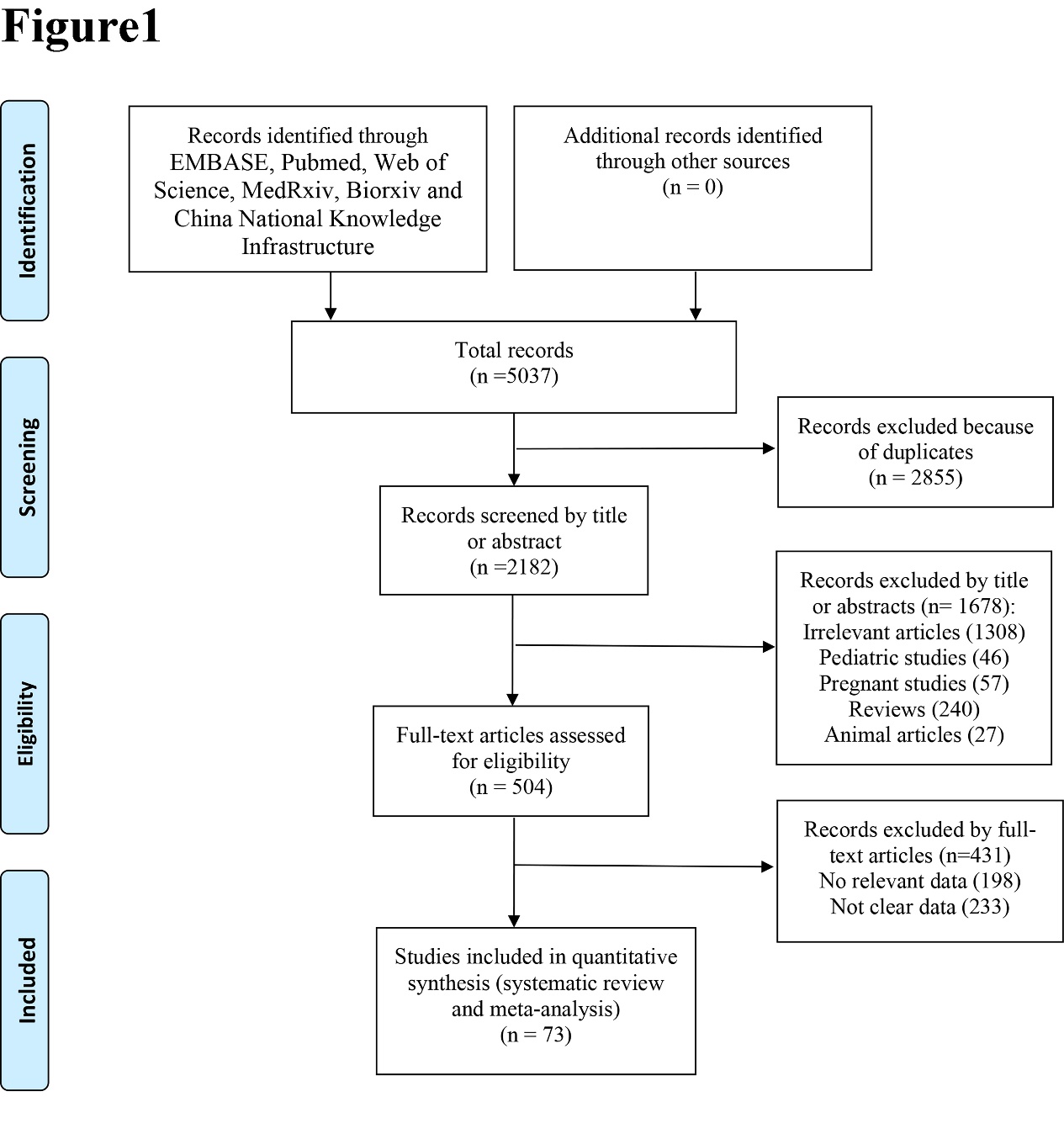
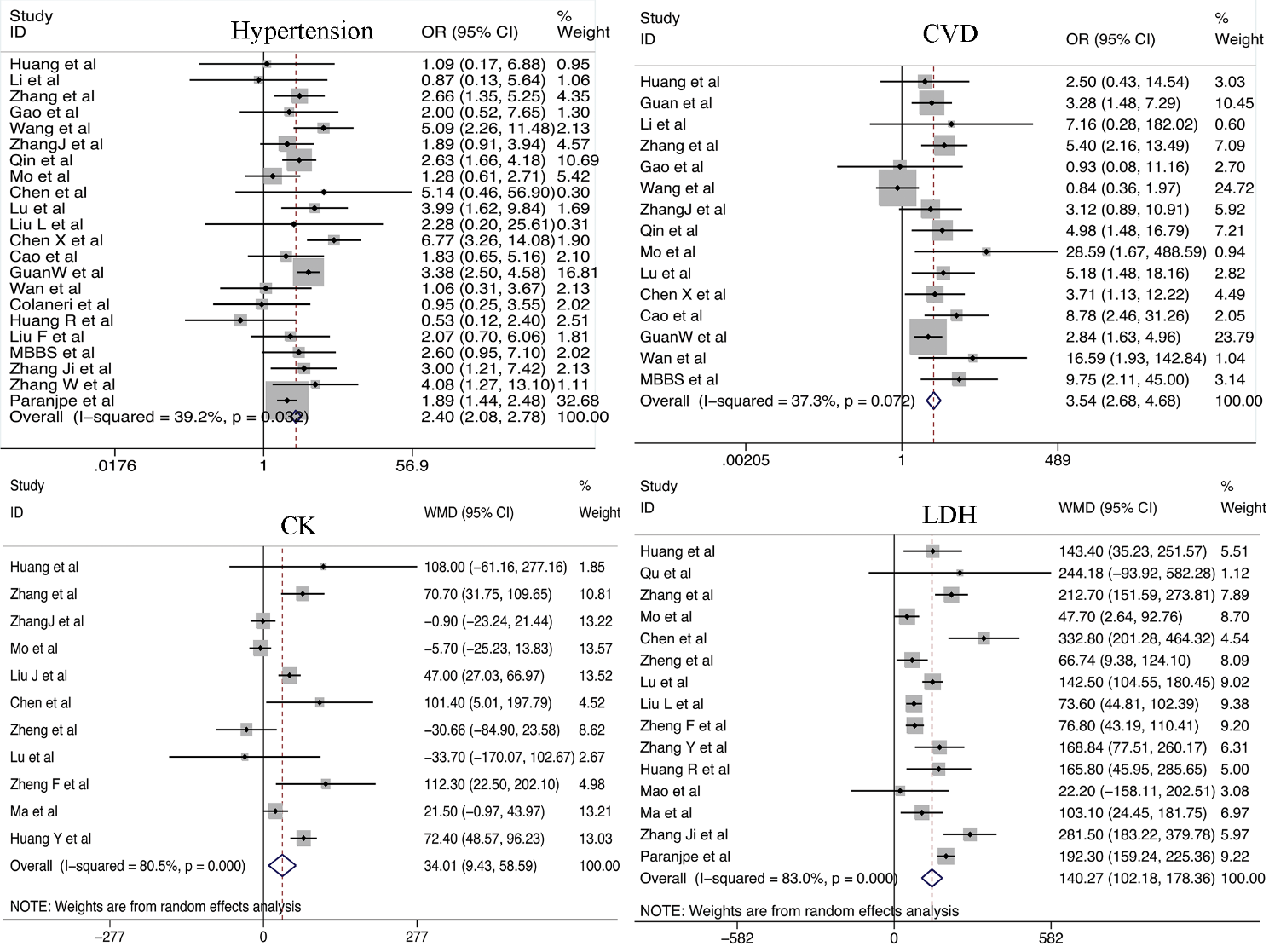
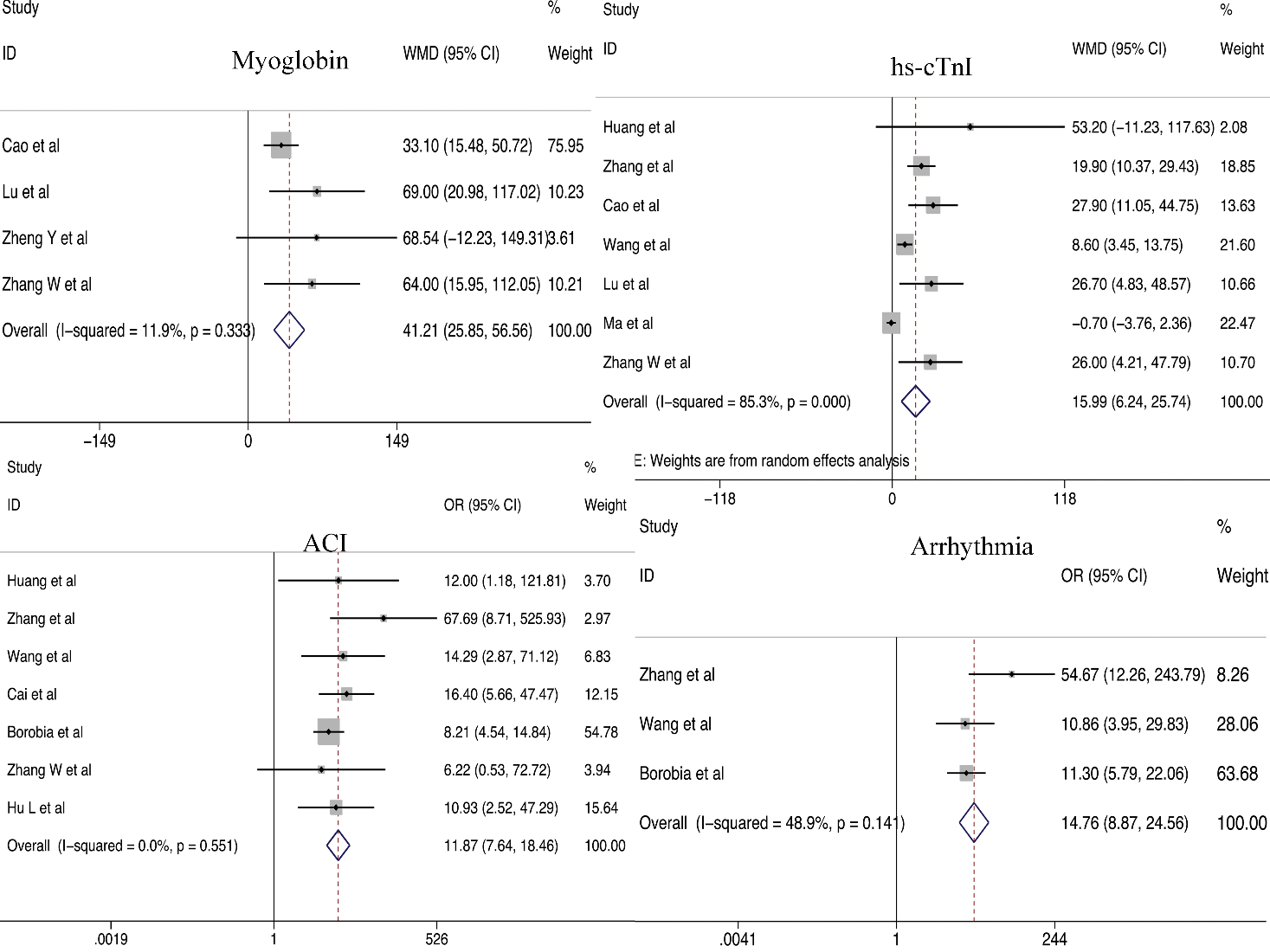
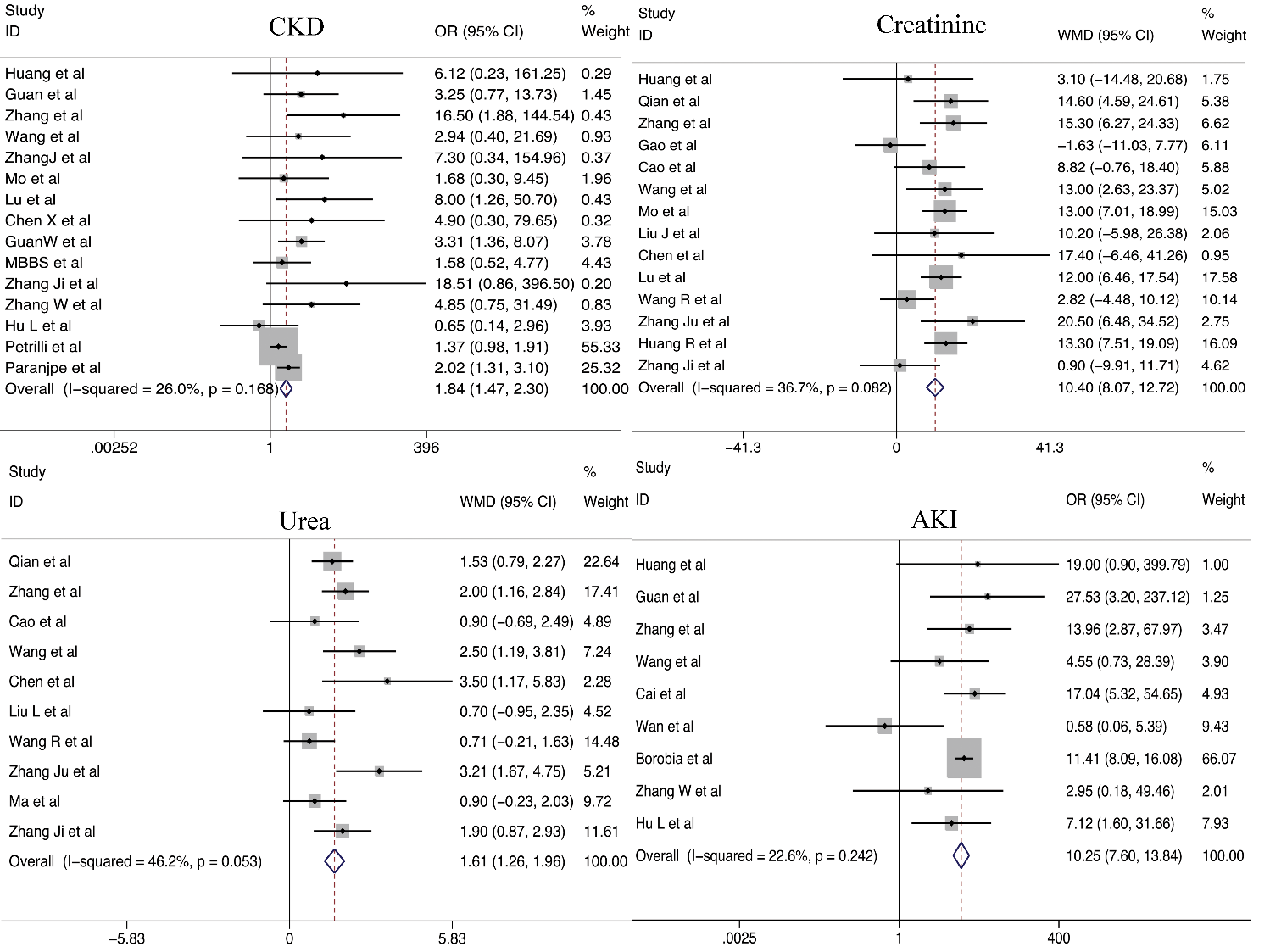
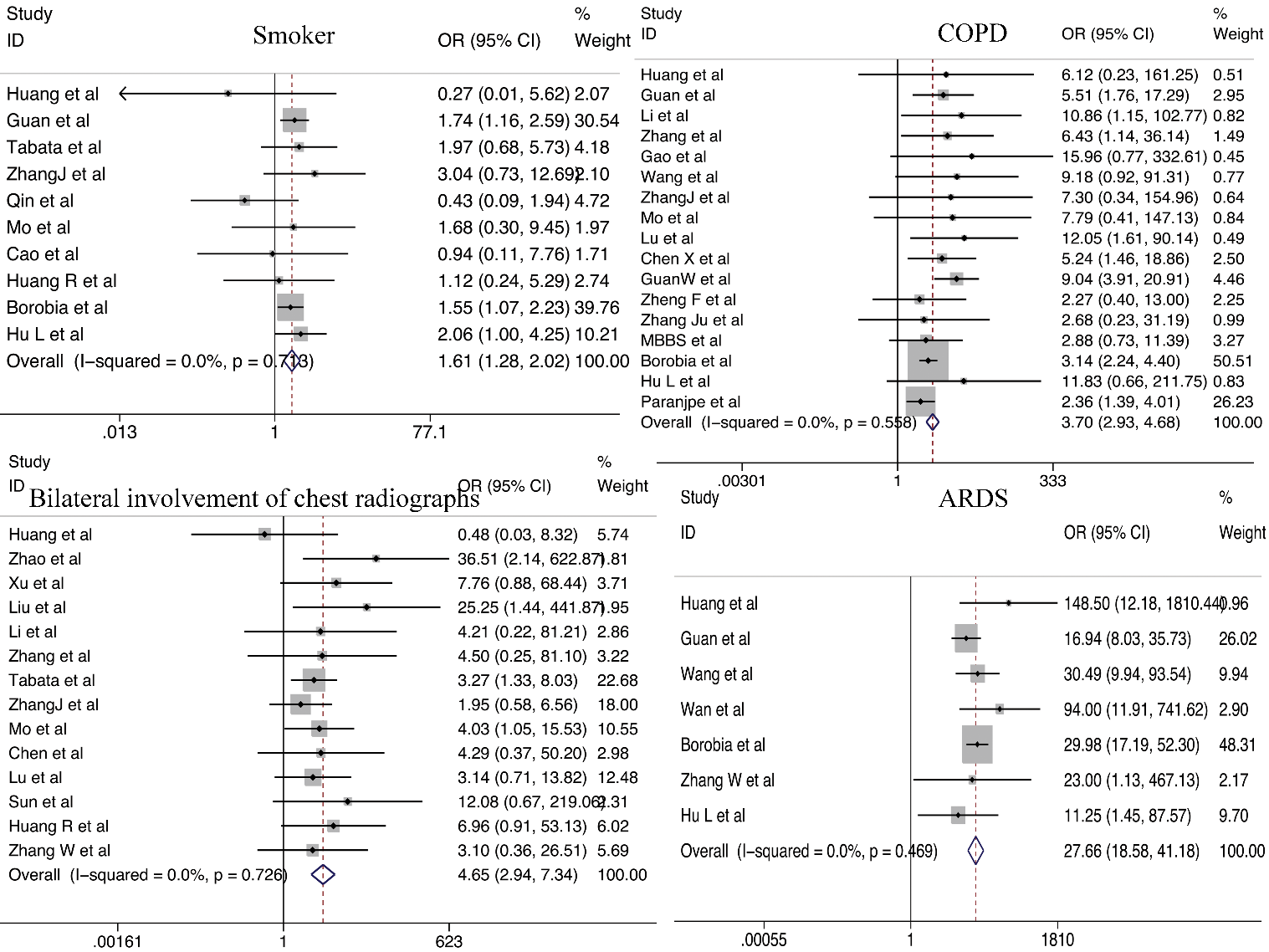
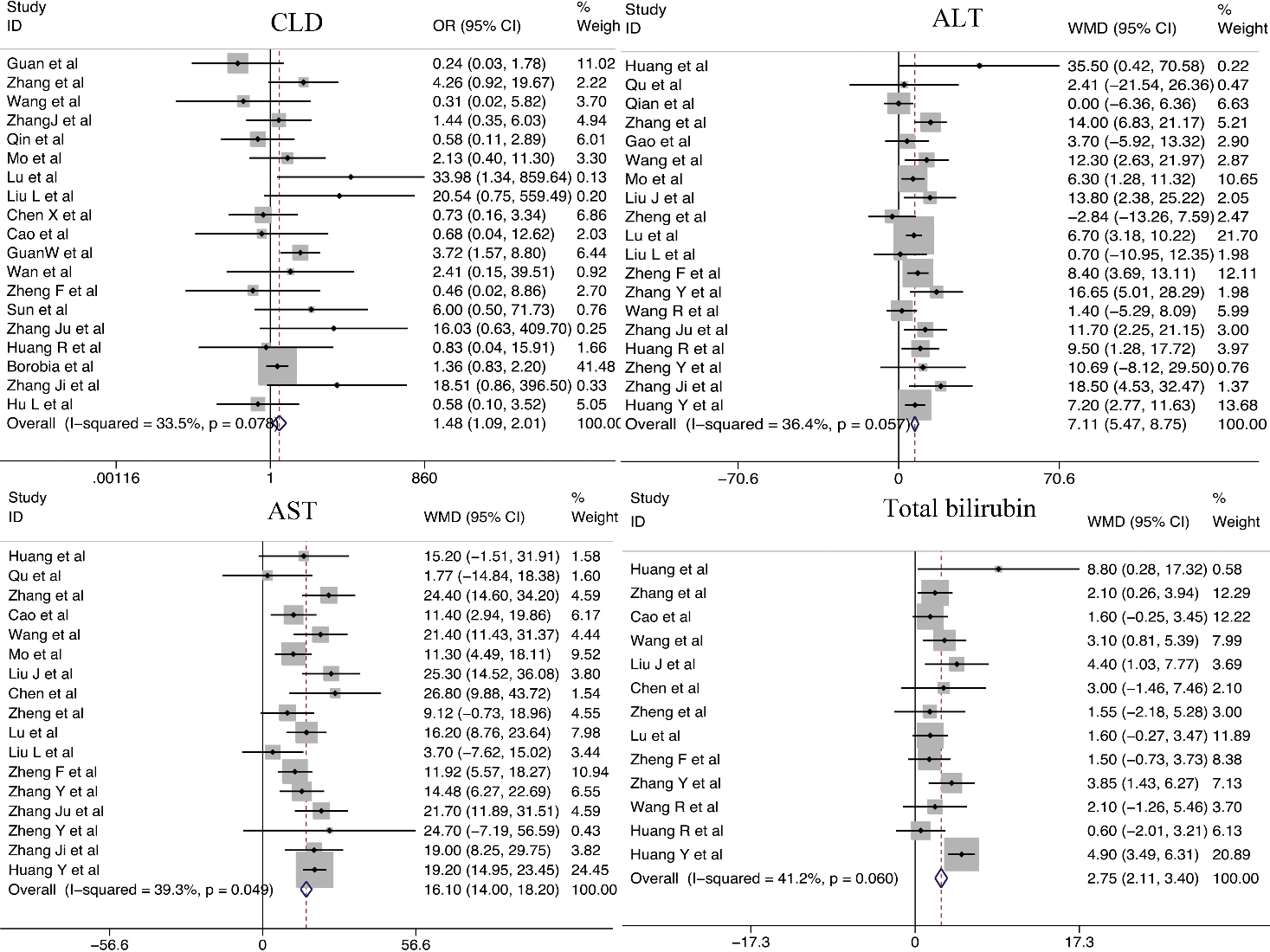
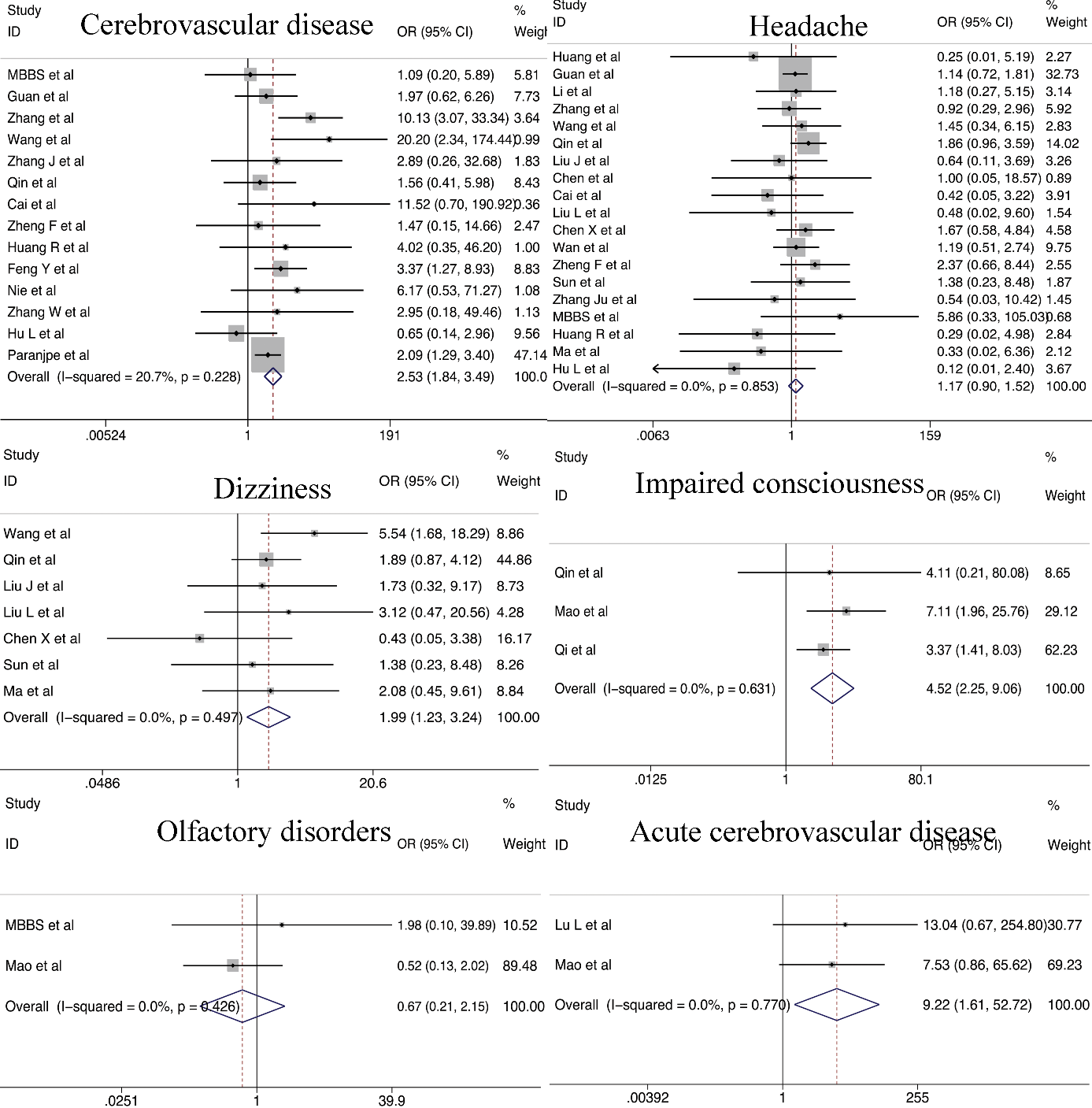
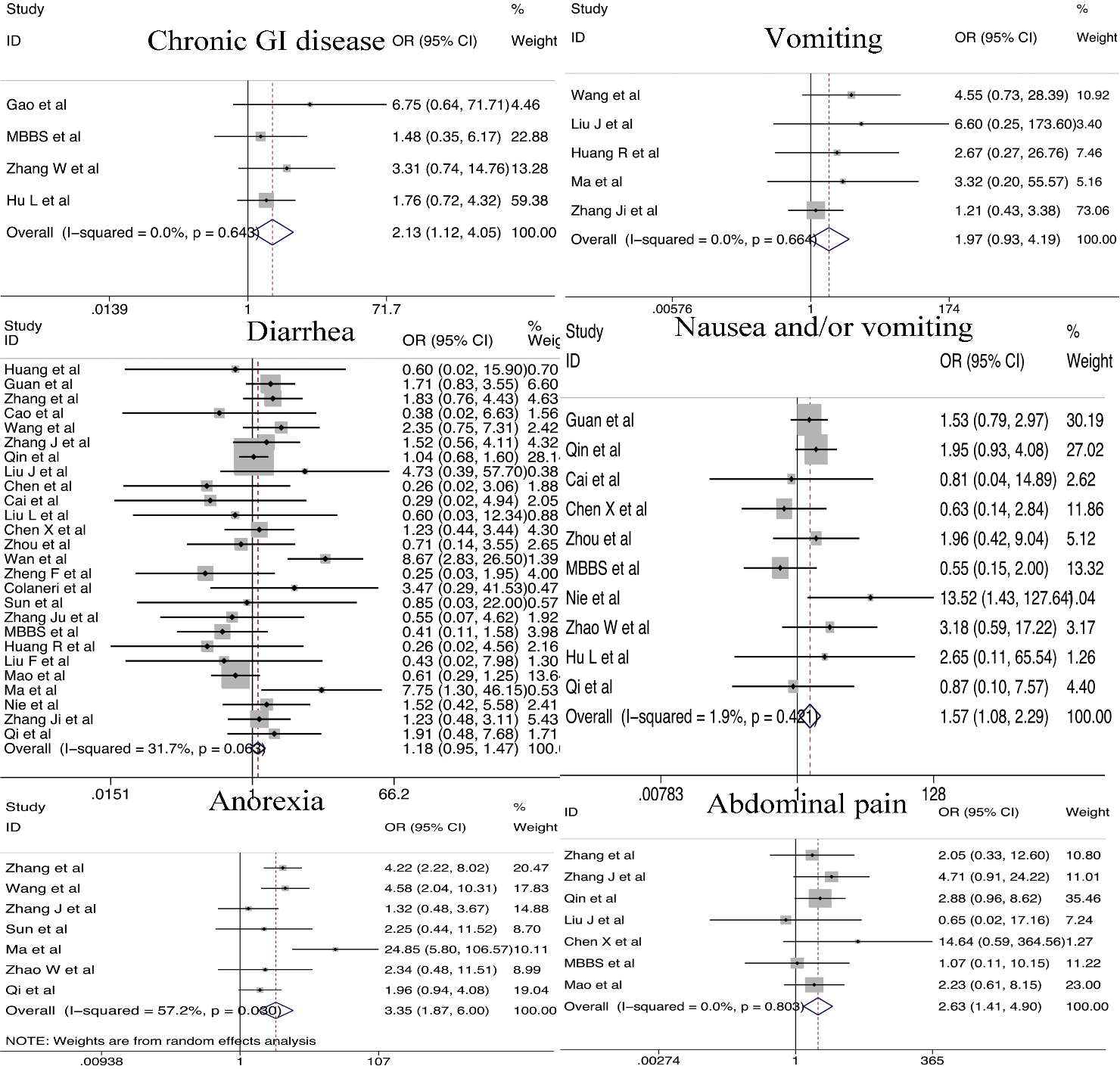
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}



